

Long-term outcomes in individuals with prolonged PR interval or first-degree atrioventricular block
- PMID: 19549974
- PMCID: PMC2765917
- DOI: 10.1001/jama.2009.888
Long-term outcomes in individuals with prolonged PR interval or first-degree atrioventricular block
Abstract
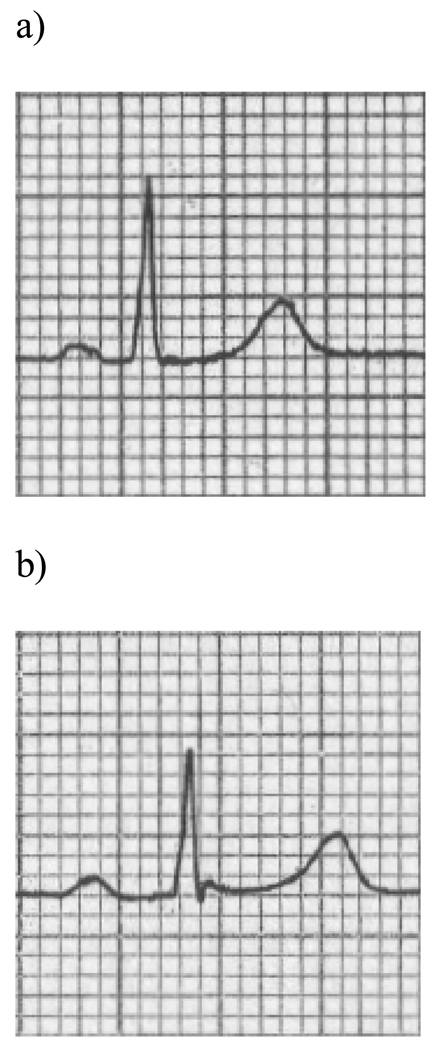
Context: Prolongation of the electrocardiographic PR interval, known as first-degree atrioventricular block when the PR interval exceeds 200 milliseconds, is frequently encountered in clinical practice.
Objective: To determine the clinical significance of PR prolongation in ambulatory individuals.
Design, setting, and participants: Prospective, community-based cohort including 7575 individuals from the Framingham Heart Study (mean age, 47 years; 54% women) who underwent routine 12-lead electrocardiography. The study cohort underwent prospective follow-up through 2007 from baseline examinations in 1968-1974. Multivariable-adjusted Cox proportional hazards models were used to examine the associations of PR interval with the incidence of arrhythmic events and death.
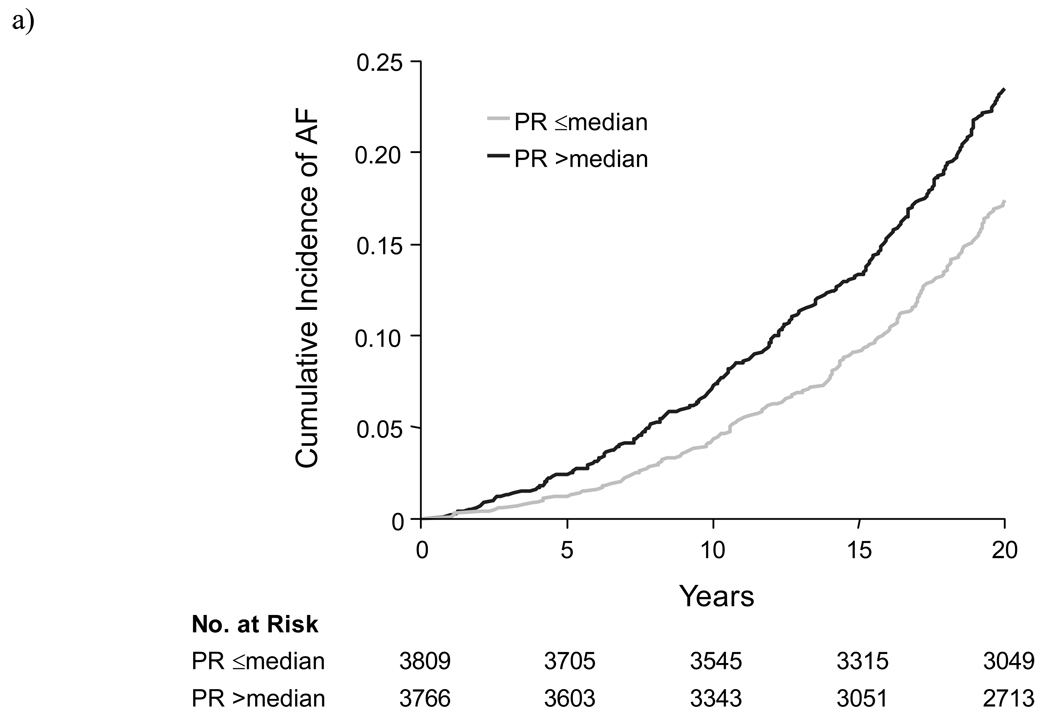
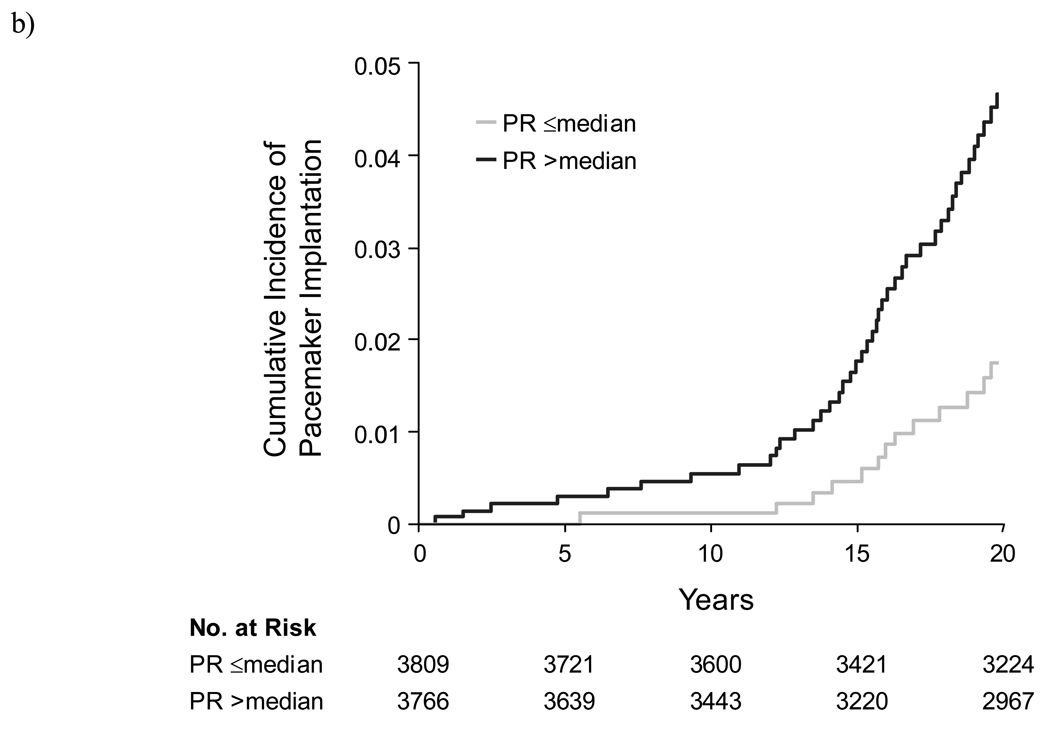
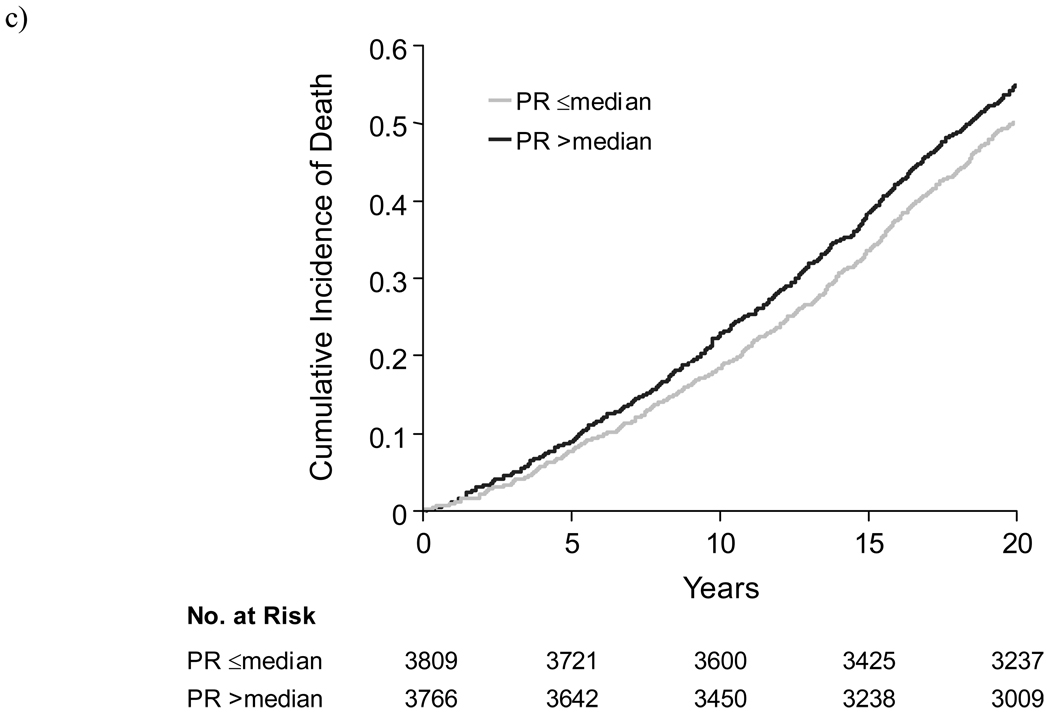
Main outcome measures: Incident atrial fibrillation (AF), pacemaker implantation, and all-cause mortality.
Results: During follow-up, 481 participants developed AF, 124 required pacemaker implantation, and 1739 died. At the baseline examination, 124 individuals had PR intervals longer than 200 milliseconds. For those with PR intervals longer than 200 milliseconds compared with those with PR intervals of 200 milliseconds or shorter, incidence rates per 10 000 person-years were 140 (95% confidence interval [CI], 95-208) vs 36 (95% CI, 32-39) for AF, 59 (95% CI, 40-87) vs 6 (95% CI, 5-7) for pacemaker implantation, and 334 (95% CI, 260-428) vs 129 (95% CI, 123-135) for all-cause mortality. Corresponding absolute risk increases were 1.04% (AF), 0.53% (pacemaker implantation), and 2.05% (all-cause mortality) per year. In multivariable analyses, each 20-millisecond increment in PR was associated with an adjusted hazard ratio (HR) of 1.11 (95% CI, 1.02-1.22; P = .02) for AF, 1.22 (95% CI, 1.14-1.30; P < .001) for pacemaker implantation, and 1.08 (95% CI, 1.02-1.13; P = .005) for all-cause mortality. Individuals with first-degree atrioventricular block had a 2-fold adjusted risk of AF (HR, 2.06; 95% CI, 1.36-3.12; P < .001), 3-fold adjusted risk of pacemaker implantation (HR, 2.89; 95% CI, 1.83-4.57; P < .001), and 1.4-fold adjusted risk of all-cause mortality (HR, 1.44, 95% CI, 1.09-1.91; P = .01).
Conclusion: Prolongation of the PR interval is associated with increased risks of AF, pacemaker implantation, and all-cause mortality.
Figures
Comment in
-
Outcomes in patients with prolonged PR interval or first-degree atrioventricular block.JAMA. 2009 Nov 11;302(18):1967; author reply 1967-8. doi: 10.1001/jama.2009.1604. JAMA. 2009. PMID: 19903912 No abstract available.
-
Outcomes in patients with prolonged PR interval or first-degree atrioventricular block.JAMA. 2009 Nov 11;302(18):1967; author reply 1967-8. doi: 10.1001/jama.2009.1603. JAMA. 2009. PMID: 19903913 No abstract available.
-
ACP Journal Club: Prolonged PR intervals were associated with increased risk for atrial fibrillation, pacemaker implantation, and mortality.Ann Intern Med. 2009 Nov 17;151(10):JC5-13. doi: 10.7326/0003-4819-151-10-200911170-02013. Ann Intern Med. 2009. PMID: 19920258 No abstract available.
References
-
- Packard JM, Graettinger JS, Graybiel A. Analysis of the electrocardiograms obtained from 1000 young healthy aviators; ten year follow-up. Circulation. 1954;10:384–400. - PubMed
-
- Blackburn H, Taylor HL, Keys A. Coronary heart disease in seven countries. XVI. The electrocardiogram in prediction of five-year coronary heart disease incidence among men aged forty through fifty-nine. Circulation. 1970;41:I154–I161. - PubMed
-
- Erikssen J, Otterstad JE. Natural course of a prolonged PR interval and the relation between PR and incidence of coronary heart disease. A 7-year follow-up study of 1832 apparently healthy men aged 40–59 years. Clin Cardiol. 1984;7:6–13. - PubMed
-
- Schwartzman D. Atrioventricular block and atrioventricular dissociation. In: Zipes D, Jalife J, editors. Cardiac Electrophysiology: From Cell to Bedside. 4th ed. Philadelphia, PA: Saunders; 2004. pp. 485–489.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
