

Factors associated with septic shock and mortality in generalized peritonitis: comparison between community-acquired and postoperative peritonitis
- PMID: 19552799
- PMCID: PMC2717471
- DOI: 10.1186/cc7931
Factors associated with septic shock and mortality in generalized peritonitis: comparison between community-acquired and postoperative peritonitis
Abstract
Introduction: The risk factors associated with poor outcome in generalized peritonitis are still debated. Our aim was to analyze clinical and bacteriological factors associated with the occurrence of shock and mortality in patients with secondary generalized peritonitis.
Methods: This was a prospective observational study involving 180 consecutive patients with secondary generalized peritonitis (community-acquired and postoperative) at a single center. We recorded peri-operative occurrence of septic shock and 30-day survival rate and analyzed their associations with patients characteristics (age, gender, SAPS II, liver cirrhosis, cancer, origin of peritonitis), and microbiological/mycological data (peritoneal fluid, blood cultures).
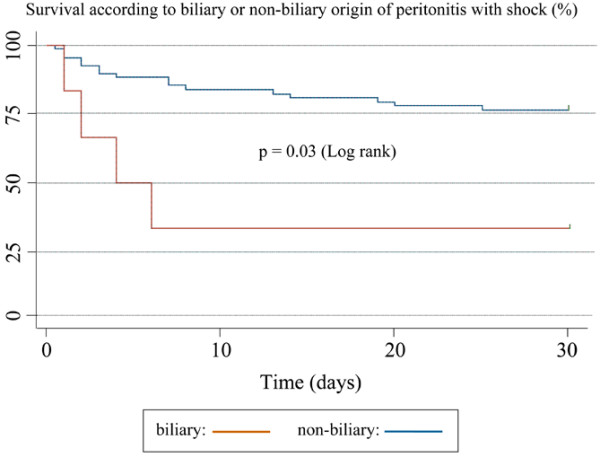
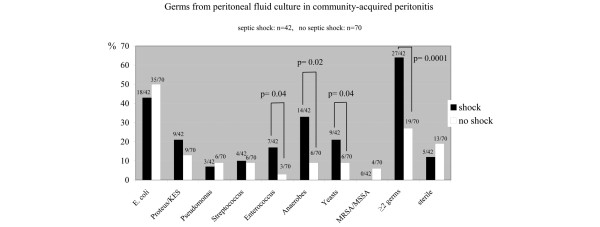
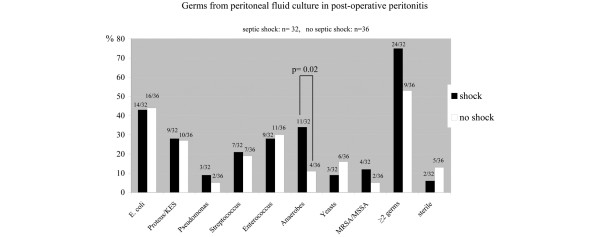
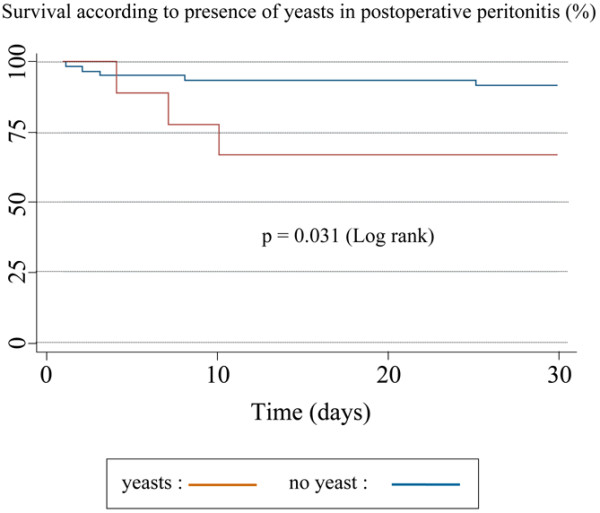
Results: Frequency of septic shock was 41% and overall mortality rate was 19% in our cohort. Patients with septic shock had a mortality rate of 35%, versus 8% for patients without shock. Septic shock occurrence and mortality rate were not different between community-acquired and postoperative peritonitis. Age over 65, two or more microorganisms, or anaerobes in peritoneal fluid culture were independent risk factors of shock. In the subgroup of peritonitis with septic shock, biliary origin was independently associated with increased mortality. In addition, intraperitoneal yeasts and Enterococci were associated with septic shock in community-acquired peritonitis. Yeasts in the peritoneal fluid of postoperative peritonitis were also an independent risk factor of death in patients with septic shock.
Conclusions: Unlike previous studies, we observed no difference in incidence of shock and prognosis between community-acquired and postoperative peritonitis. Our findings support the deleterious role of Enterococcus species and yeasts in peritoneal fluid, reinforcing the need for prospective trials evaluating systematic treatment against these microorganisms in patients with secondary peritonitis.
Figures
References
-
- Montravers P, Gauzit R, Muller C, Marmuse JP, Fichelle A, Desmonts JM. Emergence of antibiotic-resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy. Clin Infect Dis. 1996;23:486–494. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
