

Trends in broad-spectrum antibiotic prescribing for children with acute otitis media in the United States, 1998-2004
- PMID: 19552819
- PMCID: PMC2711950
- DOI: 10.1186/1471-2431-9-41
Trends in broad-spectrum antibiotic prescribing for children with acute otitis media in the United States, 1998-2004
Abstract
Background: Overuse of broad-spectrum antibiotics is associated with antibiotic resistance. Acute otitis media (AOM) is responsible for a large proportion of antibiotics prescribed for US children. Rates of broad-spectrum antibiotic prescribing for AOM are unknown.
Methods: Analysis of the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey, 1998 to 2004 (N = 6,878). Setting is office-based physicians, hospital outpatient departments, and emergency departments. Patients are children aged 12 years and younger prescribed antibiotics for acute otitis media. Main outcome measure is percentage of broad-spectrum antibiotics, defined as amoxicillin/clavulanate, macrolides, cephalosporins and quinolones.
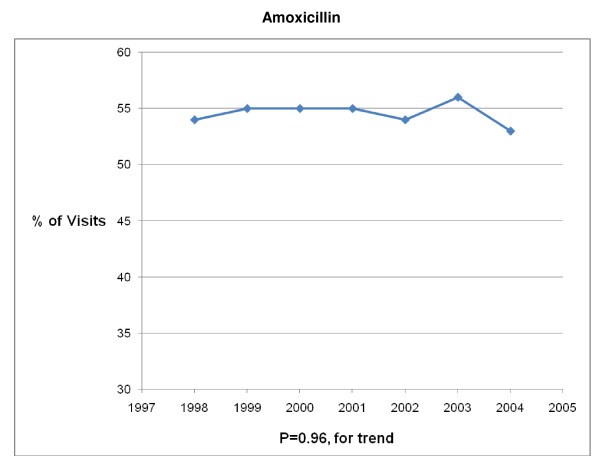
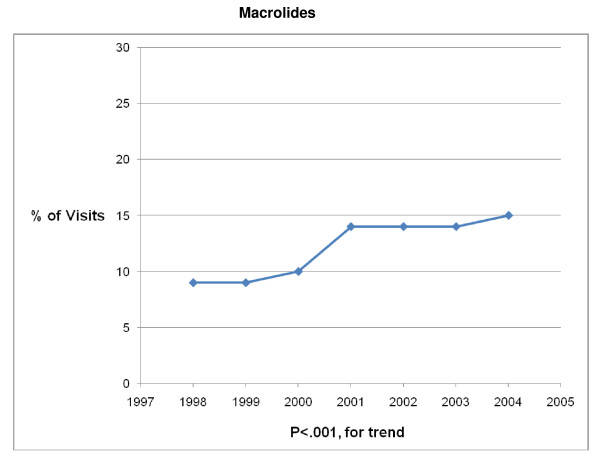
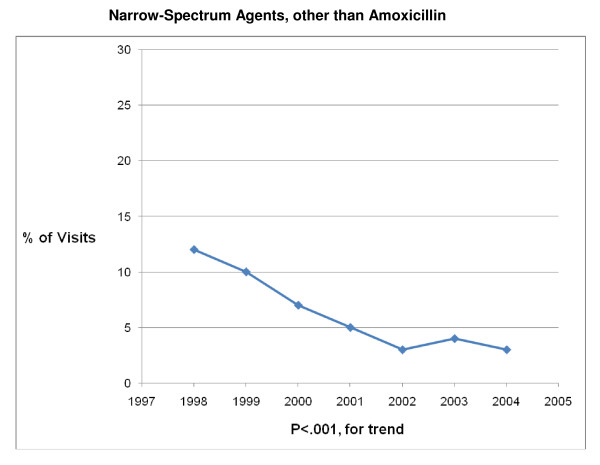
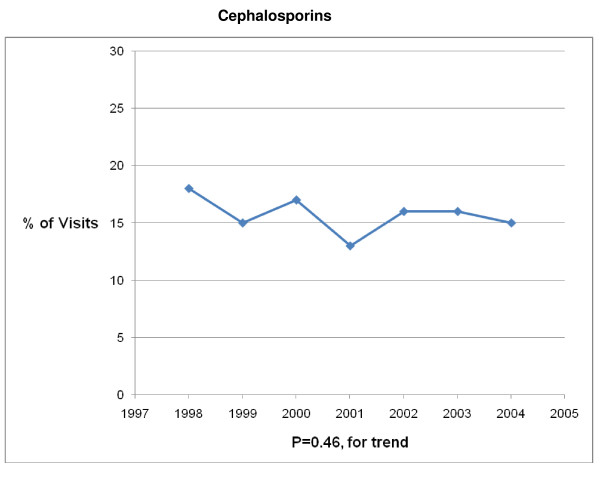
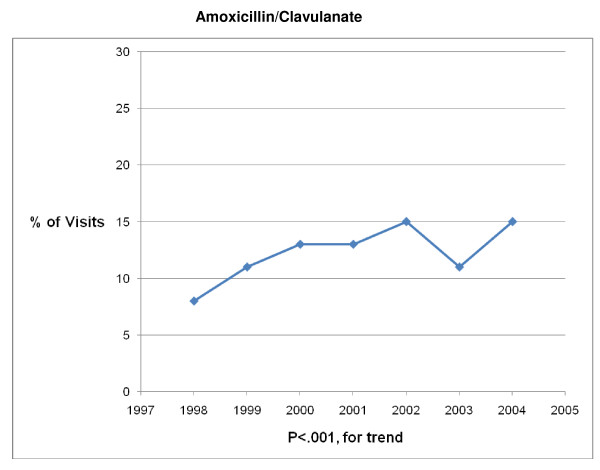
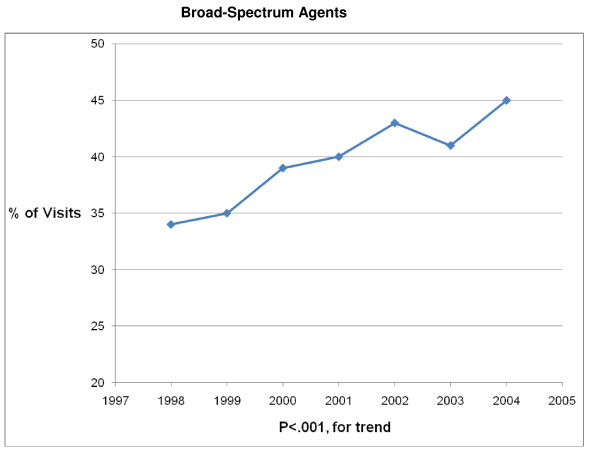
Results: Broad-spectrum prescribing for acute otitis media increased from 34% of visits in 1998 to 45% of visits in 2004 (P < .001 for trend). The trend was primarily attributable to an increase in prescribing of amoxicillin/clavulanate (8% to 15%; P < .001 for trend) and macrolides (9% to 15%; P < .001 for trend). Prescribing remained stable for amoxicillin and cephalosporins while decreasing for narrow-spectrum agents (12% to 3%; P < .001 for trend) over the study period. Independent predictors of broad-spectrum antibiotic prescribing were ear pain, non-white race, public and other insurance (compared to private), hospital outpatient department setting, emergency department setting, and West region (compared to South and Midwest regions), each of which was associated with lower rates of broad-spectrum prescribing. Age and fever were not associated with prescribing choice.
Conclusion: Prescribing of broad-spectrum antibiotics for acute otitis media has steadily increased from 1998 to 2004. Associations with non-clinical factors suggest potential for improvement in prescribing practice.
Figures
References
-
- Goosens H, Ferech M, Stichele R Vander, Elseviers M, for the ESAC Project Group Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365:579–587. - PubMed
-
- Spellberg B, Guidos R, Gilbert D, Bradley J, Boucher HW, Scheld WM, Bartlett JG, Edwards J., Jr The epidemic of antibiotic-resistant infections: a call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:155–164. doi: 10.1086/524891. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
