

Screening men for abdominal aortic aneurysm: 10 year mortality and cost effectiveness results from the randomised Multicentre Aneurysm Screening Study
- PMID: 19553269
- PMCID: PMC3272658
- DOI: 10.1136/bmj.b2307
Screening men for abdominal aortic aneurysm: 10 year mortality and cost effectiveness results from the randomised Multicentre Aneurysm Screening Study
Abstract
Objectives: To assess whether the mortality benefit from screening men aged 65-74 for abdominal aortic aneurysm decreases over time, and to estimate the long term cost effectiveness of screening.
Design: Randomised trial with 10 years of follow-up.
Setting: Four centres in the UK. Screening and surveillance was delivered mainly in primary care settings, with follow-up and surgery offered in hospitals.
Participants: Population based sample of 67 770 men aged 65-74.
Interventions: Participants were individually allocated to invitation to ultrasound screening (invited group) or to a control group not offered screening. Patients with an abdominal aortic aneurysm detected at screening underwent surveillance and were offered surgery if they met predefined criteria.
Main outcome measures: Mortality and costs related to abdominal aortic aneurysm, and cost per life year gained.
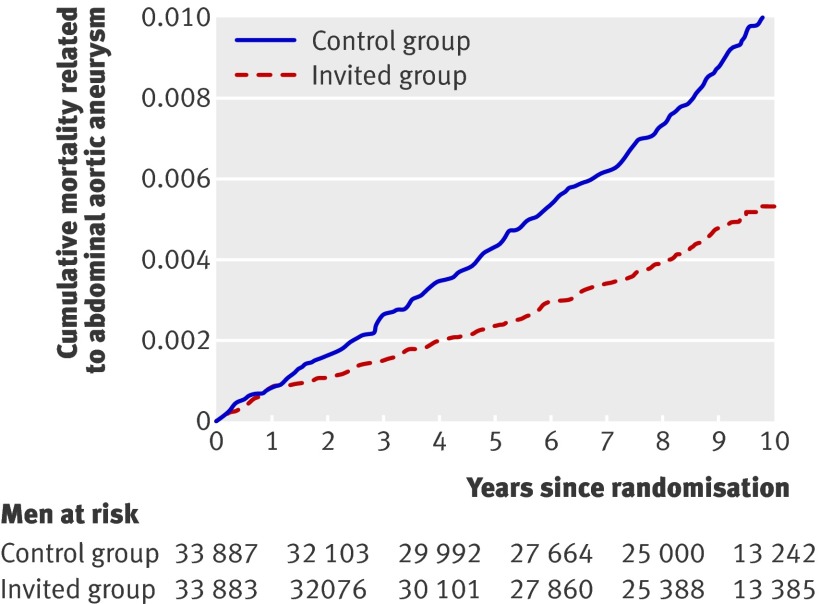
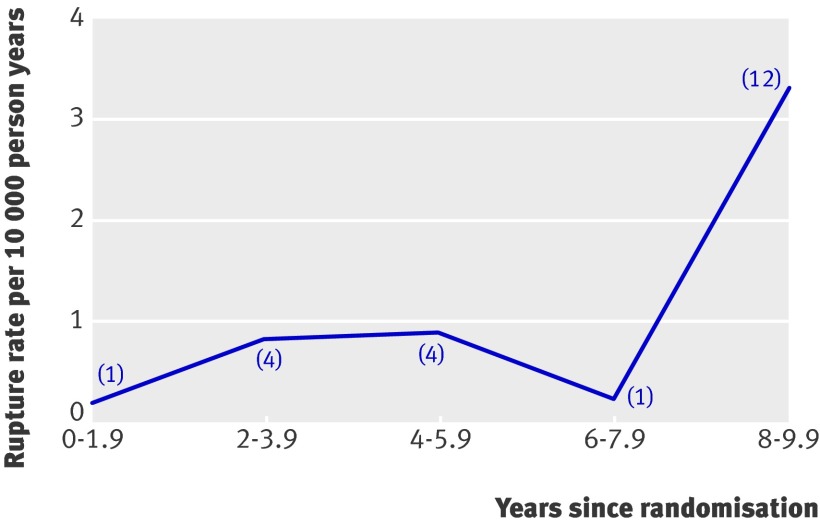
Results: Over 10 years 155 deaths related to abdominal aortic aneurysm (absolute risk 0.46%) occurred in the invited group and 296 (0.87%) in the control group (relative risk reduction 48%, 95% confidence interval 37% to 57%). The degree of benefit seen in earlier years of follow-up was maintained in later years. Based on the 10 year trial data, the incremental cost per man invited to screening was pound100 (95% confidence interval pound82 to pound118), leading to an incremental cost effectiveness ratio of pound7600 ( pound5100 to pound13,000) per life year gained. However, the incidence of ruptured abdominal aortic aneurysms in those originally screened as normal increased noticeably after eight years.
Conclusions: The mortality benefit of screening men aged 65-74 for abdominal aortic aneurysm is maintained up to 10 years and cost effectiveness becomes more favourable over time. To maximise the benefit from a screening programme, emphasis should be placed on achieving a high initial rate of attendance and good adherence to clinical follow-up, preventing delays in undertaking surgery, and maintaining a low operative mortality after elective surgery. On the basis of current evidence, rescreening of those originally screened as normal is not justified. Trial registration Current Controlled Trials ISRCTN37381646.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Screening for abdominal aortic aneurysm.BMJ. 2009 Jun 24;338:b2185. doi: 10.1136/bmj.b2185. BMJ. 2009. PMID: 19553266 No abstract available.
-
ACP Journal Club: Screening for abdominal aortic aneurysm (AAA) in men 65 to 74 years of age was cost-effective for AAA mortality at 10 years.Ann Intern Med. 2009 Nov 17;151(10):JC5-15. doi: 10.7326/0003-4819-151-10-200911170-02015. Ann Intern Med. 2009. PMID: 19920260 No abstract available.
References
-
- UK National Screening Committee. Abdominal aortic aneurysm screening, May 2007. 2008. www.library.nhs.uk/screening/.
-
- NHS National Services Scotland. Abdominal aortic aneurysm (AAA) screening, Aug 2008. www.nhsnss.org/uploads/board_papers/B0893%20AAAScreening.pdf.
-
- US Preventive Services Task Force. Screening for abdominal aortic aneurysm: recommendation statement. Ann Intern Med 2005;142:198-202. - PubMed
-
- Multicentre Aneurysm Screening Study Group. The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomised controlled trial. Lancet 2002;360:1531-9. - PubMed
-
- Kim LG, Scott RAP, Ashton HA, Thompson SG. A sustained mortality benefit from screening for abdominal aortic aneurysm. Ann Intern Med 2007;146:699-706. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous