

An economic evaluation of venous thromboembolism prophylaxis strategies in critically ill trauma patients at risk of bleeding
- PMID: 19554085
- PMCID: PMC2695771
- DOI: 10.1371/journal.pmed.1000098
An economic evaluation of venous thromboembolism prophylaxis strategies in critically ill trauma patients at risk of bleeding
Abstract
Background: Critically ill trauma patients with severe injuries are at high risk for venous thromboembolism (VTE) and bleeding simultaneously. Currently, the optimal VTE prophylaxis strategy is unknown for trauma patients with a contraindication to pharmacological prophylaxis because of a risk of bleeding.
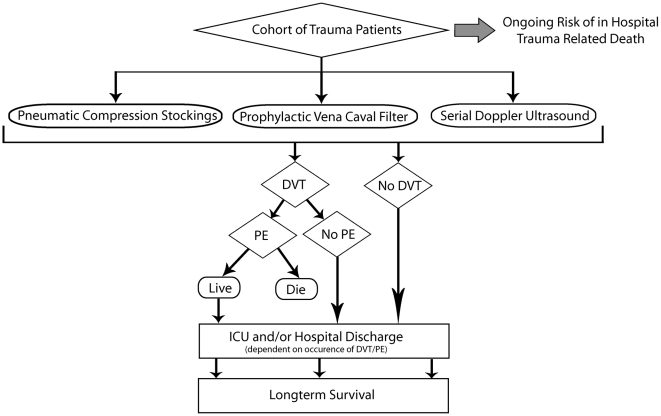
Methods and findings: Using decision analysis, we estimated the cost effectiveness of three VTE prophylaxis strategies-pneumatic compression devices (PCDs) and expectant management alone, serial Doppler ultrasound (SDU) screening, and prophylactic insertion of a vena cava filter (VCF) -- in trauma patients admitted to an intensive care unit (ICU) with severe injuries who were believed to have a contraindication to pharmacological prophylaxis for up to two weeks because of a risk of major bleeding. Data on the probability of deep vein thrombosis (DVT) and pulmonary embolism (PE), and on the effectiveness of the prophylactic strategies, were taken from observational and randomized controlled studies. The probabilities of in-hospital death, ICU and hospital discharge rates, and resource use were taken from a population-based cohort of trauma patients with severe injuries (injury severity scores >12) admitted to the ICU of a regional trauma centre. The incidence of DVT at 12 weeks was similar for the PCD (14.9%) and SDU (15.0%) strategies, but higher for the VCF (25.7%) strategy. Conversely, the incidence of PE at 12 weeks was highest in the PCD strategy (2.9%), followed by the SDU (1.5%) and VCF (0.3%) strategies. Expected mortality and quality-adjusted life years were nearly identical for all three management strategies. Expected health care costs at 12 weeks were Can$55,831 for the PCD strategy, Can$55,334 for the SDU screening strategy, and Can$57,377 for the VCF strategy, with similar trends noted over a lifetime analysis.
Conclusions: The attributable mortality due to PE in trauma patients with severe injuries is low relative to other causes of mortality. Prophylactic placement of VCF in patients at high risk of VTE who cannot receive pharmacological prophylaxis is expensive and associated with an increased risk of DVT. Compared to the other strategies, SDU screening was associated with better clinical outcomes and lower costs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Prophylaxis against venous thromboembolism in orthopedic surgery.Chin J Traumatol. 2006 Aug;9(4):249-56. Chin J Traumatol. 2006. PMID: 16849000 Review.
-
Risk factors for venous thromboembolism in critically ill trauma patients who cannot receive chemical prophylaxis.Injury. 2013 Jan;44(1):80-5. doi: 10.1016/j.injury.2011.10.006. Epub 2011 Nov 1. Injury. 2013. PMID: 22047757
-
Routine prophylactic vena cava filtration is not indicated after acute spinal cord injury.J Trauma. 2002 May;52(5):902-6. doi: 10.1097/00005373-200205000-00013. J Trauma. 2002. PMID: 11988656
-
Cost-effectiveness of guidelines for insertion of inferior vena cava filters in high-risk trauma patients.J Vasc Surg. 2010 Dec;52(6):1537-45.e1-2. doi: 10.1016/j.jvs.2010.06.152. Epub 2010 Sep 16. J Vasc Surg. 2010. PMID: 20843631
-
Deep Vein Thrombosis in Intensive Care.Adv Exp Med Biol. 2017;906:167-181. doi: 10.1007/5584_2016_114. Adv Exp Med Biol. 2017. PMID: 27628009 Review.
Cited by
-
Association between delirium in the intensive care unit and subsequent neuropsychiatric disorders.Crit Care. 2020 Jul 31;24(1):476. doi: 10.1186/s13054-020-03193-x. Crit Care. 2020. PMID: 32736572 Free PMC article.
-
Sedation strategy and ICU delirium: a multicentre, population-based propensity score-matched cohort study.BMJ Open. 2021 Jul 20;11(7):e045087. doi: 10.1136/bmjopen-2020-045087. BMJ Open. 2021. PMID: 34285003 Free PMC article.
-
Natural language processing to measure the frequency and mode of communication between healthcare professionals and family members of critically ill patients.J Am Med Inform Assoc. 2021 Mar 1;28(3):541-548. doi: 10.1093/jamia/ocaa263. J Am Med Inform Assoc. 2021. PMID: 33201981 Free PMC article.
-
Deep vein thrombosis prophylaxis in trauma patients.Thrombosis. 2011;2011:505373. doi: 10.1155/2011/505373. Epub 2011 May 15. Thrombosis. 2011. PMID: 22084663 Free PMC article.
-
Single-Stage Surgical Treatment of Acute Type A Aortic Dissection and Blunt Abdominal Trauma: A Case Report.Ann Vasc Dis. 2023 Sep 25;16(3):238-241. doi: 10.3400/avd.cr.23-00017. Ann Vasc Dis. 2023. PMID: 37779648 Free PMC article.
References
-
- Rogers FB, Cipolle MD, Velmahos G, Rozycki G, Luchette FA. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST practice management guidelines work group. J Trauma. 2002;53:142–164. - PubMed
-
- Geerts WH, Code KI, Jay RM, Chen E, Szalai JP. A prospective study of venous thromboembolism after major trauma. N Engl J Med. 1994;331:1601–1606. - PubMed
-
- Kelly J, Hunt BJ. Do anticoagulants improve survival in patients presenting with venous thromboembolism? J Intern Med. 2003;254:527–539. - PubMed
-
- Carson JL, Kelley MA, Duff A, Weg JG, Fulkerson WJ, et al. The clinical course of pulmonary embolism. N Engl J Med. 1992;326:1240–1245. - PubMed
-
- Geerts WH. Prevention of venous thromboembolism in high-risk patients. Hematology Am Soc Hematol Educ Program. 2006. pp. 462–466. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
