

Wound care in the geriatric client
- PMID: 19554098
- PMCID: PMC2697592
- DOI: 10.2147/cia.s4726
Wound care in the geriatric client
Abstract
With our aging population, chronic diseases that compromise skin integrity such as diabetes, peripheral vascular disease (venous hypertension, arterial insufficiency) are becoming increasingly common. Skin breakdown with ulcer and chronic wound formation is a frequent consequence of these diseases. Types of ulcers include pressure ulcers, vascular ulcers (arterial and venous hypertension), and neuropathic ulcers. Treatment of these ulcers involves recognizing the four stages of healing: coagulation, inflammation, proliferation, and maturation. Chronic wounds are frequently stalled in the inflammatory stage. Moving past the inflammation stage requires considering the bacterial burden, necrotic tissue, and moisture balance of the wound being treated. Bacterial overgrowth or infection needs to be treated with topical or systemic agents. In most cases, necrotic tissue needs to be debrided and moisture balance needs to be addressed by wetting dry tissue and drying wet tissue. Special dressings have been developed to accomplish these tasks. They include films, hydrocolloids, hydrogel dressings, foams, hydrofibers, composite and alginate dressings.
Keywords: debridement; diabetic ulcers; elderly; pressure ulcers; vascular ulcers; wound care.
Figures











Similar articles
-
Wound care in venous ulcers.Phlebology. 2013 Mar;28 Suppl 1:79-85. doi: 10.1177/0268355513477015. Phlebology. 2013. PMID: 23482540 Review.
-
Management of chronic pressure ulcers: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(3):1-203. Epub 2009 Jul 1. Ont Health Technol Assess Ser. 2009. PMID: 23074533 Free PMC article.
-
[DRESSINGS FOR CHRONIC WOUNDS TREATMENT]].Acta Med Croatica. 2016;70 Suppl 1:69-77. Acta Med Croatica. 2016. PMID: 29087675 Review. Croatian.
-
Negative pressure wound therapy: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(14):1-38. Epub 2006 Jul 1. Ont Health Technol Assess Ser. 2006. PMID: 23074484 Free PMC article.
-
Factors influencing pressure ulcer healing in adults over 50: an exploratory study.J Am Med Dir Assoc. 2007 Jul;8(6):378-87. doi: 10.1016/j.jamda.2007.02.011. Epub 2007 Jun 14. J Am Med Dir Assoc. 2007. PMID: 17619036
Cited by
-
Economic evaluations of guideline-based or strategic interventions for the prevention or treatment of chronic wounds.Appl Health Econ Health Policy. 2014 Aug;12(4):373-89. doi: 10.1007/s40258-014-0094-9. Appl Health Econ Health Policy. 2014. PMID: 24615160 Free PMC article. Review.
-
Low Cost Inkjet Printed Smart Bandage for Wireless Monitoring of Chronic Wounds.Sci Rep. 2016 Jun 29;6:28949. doi: 10.1038/srep28949. Sci Rep. 2016. PMID: 27353200 Free PMC article.
-
Accuracy of digital measurement for quantitative and qualitative indicators of wound healing and repair: a systematic review protocol.BMJ Open. 2024 May 31;14(5):e085969. doi: 10.1136/bmjopen-2024-085969. BMJ Open. 2024. PMID: 38821568 Free PMC article.
-
On the Cutting Edge: Wound Care for the Endovascular Specialist.Semin Intervent Radiol. 2018 Dec;35(5):406-426. doi: 10.1055/s-0038-1676342. Epub 2019 Feb 5. Semin Intervent Radiol. 2018. PMID: 30728657 Free PMC article. Review.
-
An artificial intelligence-enabled smartphone app for real-time pressure injury assessment.Front Med Technol. 2022 Sep 23;4:905074. doi: 10.3389/fmedt.2022.905074. eCollection 2022. Front Med Technol. 2022. PMID: 36212608 Free PMC article.
References
-
- Thomas DR. Issues and dilemmas in prevention and treatment of pressure ulcers: a review. J Gerontol. 2001;56A:M328–M340. - PubMed
-
- Stotts N. Facilitating positive outcomes in older adults with wounds. Nurs Clin North Am. 2005;40:267–279. - PubMed
-
- Langemo DK. Skin fails too: acute, chronic, and end-stage skin failure. Adv Skin Wound Care. 2006;19:206–211. - PubMed
-
- Shea JD. Pressure sores classification and management. Clin Orthop Relat Res. 1975;112:89–100. - PubMed
-
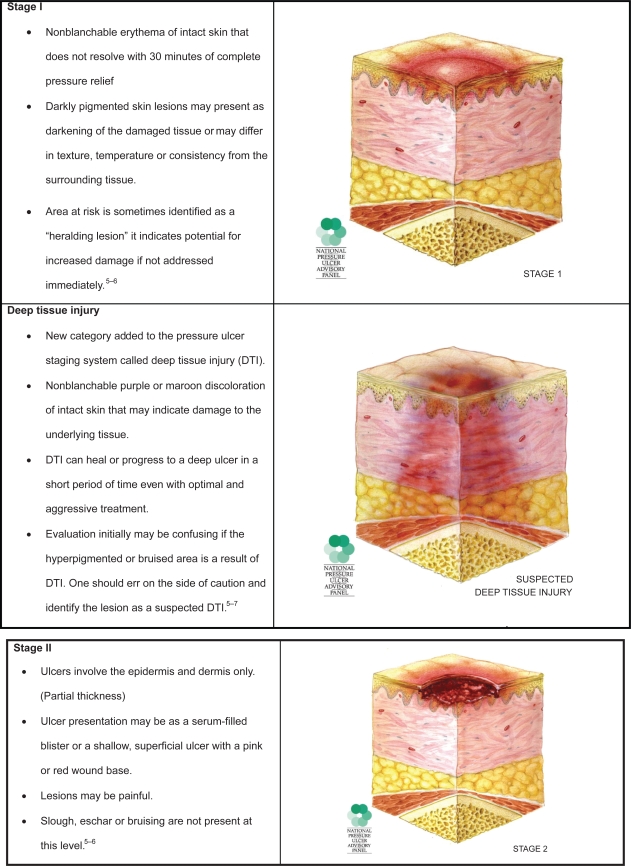
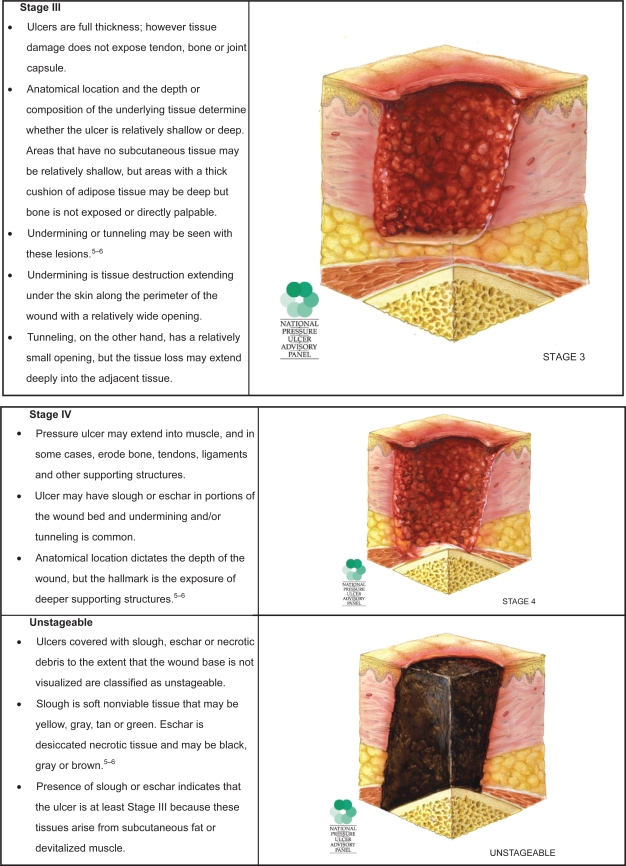
- Black J, et al. National Pressure Ulcer Advisory Panel National Pressure Ulcer Advisory Panel’s updated pressure ulcer staging system. Dermatol Nurs. 2007;19:343–349. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
