

Breast autoaugmentation
- PMID: 19554189
- PMCID: PMC2698805
- DOI: 10.1177/229255030701500201
Breast autoaugmentation
Abstract
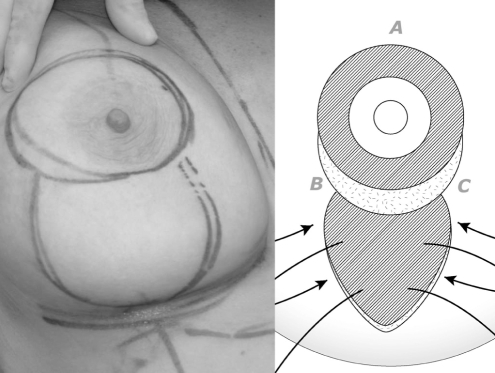
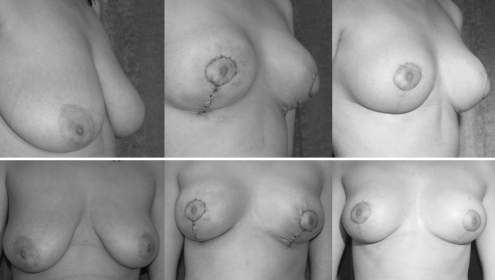
A technique using a posteriorly based dermoglandular flap as an augmentation of the superior hemisphere of the breast combined with a periareolar mastopexy and vertical mastopexy is presented. The advantages of combining a periareolar mastopexy, in terms of reducing the length of the vertical scar and preventing areolar distortion, are explained.
On présente ici une technique qui repose sur l’utilisation d’un lambeau dermoglandulaire postérieur pour l’augmentation de l’hémisphère supérieur du sein, combinée à une mastopexie périaréolaire et à une mastopexie verticale. On explique les avantages de combiner une mastopexie périaérolaire, qui permet de réduire la longueur de la cicatrice verticale et de prévenir la distorsion de l’aréole.
Keywords: Augmentation; Mastopexy; Periareolar; Ptosis; Vertical.
Figures



References
-
- Graf R, Reis de Araujo LR, Rippel R, Neto LG, Pace DT, Biggs T. Reduction mammaplasty and mastopexy using the vertical scar and thoracic wall flap technique. Aesthetic Plast Surg. 2003;27:6–12. - PubMed
-
- Botti G. Vertical scar mammaplasty: Stable padding of the superior pole by means of posteriorly based pedicle autoprosthesis. Aesthetic Surg J. 1999;19:116–23.
-
- Lejour M. Vertical mammaplasty: Early complications after 250 personal consecutive cases. Plast Reconstr Surg. 1999;104:764–70. - PubMed
-
- Lassus C. A 30-year experience with vertical mammaplasty. Plast Reconstr Surg. 1996;97:373–80. - PubMed
LinkOut - more resources
Full Text Sources