

Acute extensive portal and mesenteric venous thrombosis after splenectomy: treated by interventional thrombolysis with transjugular approach
- PMID: 19554658
- PMCID: PMC2702113
- DOI: 10.3748/wjg.15.3038
Acute extensive portal and mesenteric venous thrombosis after splenectomy: treated by interventional thrombolysis with transjugular approach
Abstract
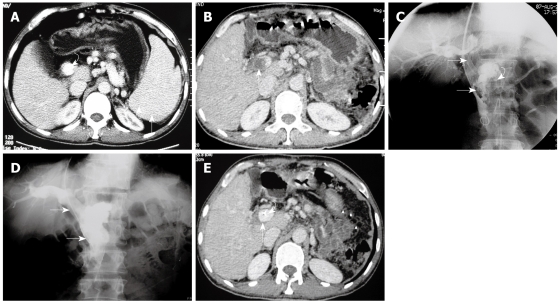
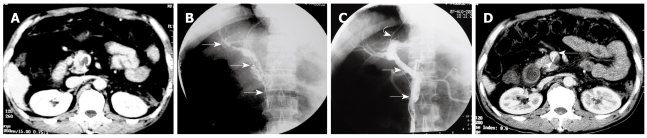
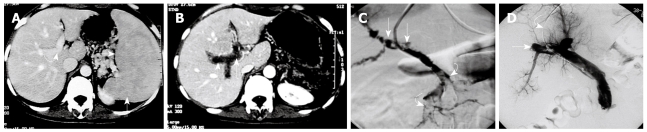
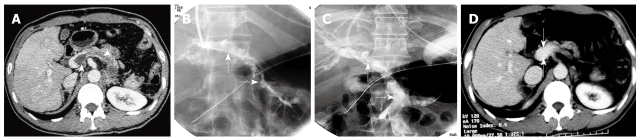
Aim: To present a series of cases with symptomatic acute extensive portal vein (PV) and superior mesenteric vein (SMV) thrombosis after splenectomy treated by transjugular intrahepatic approach catheter-directed thrombolysis.
Methods: A total of 6 patients with acute extensive PV-SMV thrombosis after splenectomy were treated by transjugular approach catheter-directed thrombolysis. The mean age of the patients was 41.2 years. After access to the portal system via the transjugular approach, pigtail catheter fragmentation of clots, local urokinase injection, and manual aspiration thrombectomy were used for the initial treatment of PV-SMV thrombosis, followed by continuous thrombolytic therapy via an indwelling infusion catheter in the SMV, which was performed for three to six days. Adequate anticoagulation was given during treatment, throughout hospitalization, and after discharge.
Results: Technical success was achieved in all 6 patients. Clinical improvement was seen in these patients within 12-24 h of the procedure. No complications were observed. The 6 patients were discharged 6-14 d (8 +/- 2.5 d) after admission. The mean duration of follow-up after hospital discharge was 40 +/- 16.5 mo. Ultrasound and contrast-enhanced computed tomography confirmed patency of the PV and SMV, and no recurrent episodes of PV-SMV thrombosis developed during the follow-up period.
Conclusion: Catheter-directed thrombolysis via transjugular intrahepatic access is a safe and effective therapy for the management of patients with symptomatic acute extensive PV-SMV thrombosis.
Figures
Similar articles
-
Acute symptomatic mesenteric venous thrombosis: treatment by catheter-directed thrombolysis with transjugular intrahepatic route.Abdom Imaging. 2011 Aug;36(4):390-8. doi: 10.1007/s00261-010-9637-1. Abdom Imaging. 2011. PMID: 20652243 Free PMC article.
-
[Transradial approach for transcatheter selective superior mesenteric artery urokinase infusion therapy in patients with acute extensive portal and superior mesenteric vein thrombosis].Zhonghua Yi Xue Za Zhi. 2012 Jun 5;92(21):1448-52. Zhonghua Yi Xue Za Zhi. 2012. PMID: 22944028 Chinese.
-
Transradial approach for transcatheter selective superior mesenteric artery urokinase infusion therapy in patients with acute extensive portal and superior mesenteric vein thrombosis.Cardiovasc Intervent Radiol. 2010 Feb;33(1):80-9. doi: 10.1007/s00270-009-9777-2. Epub 2009 Dec 22. Cardiovasc Intervent Radiol. 2010. PMID: 20033163
-
Acute Mesenteric and Portal Vein Thrombosis: Etiology, Diagnosis, and Interventional Management.Tech Vasc Interv Radiol. 2025 Sep;28(3):101058. doi: 10.1016/j.tvir.2025.101058. Epub 2025 Jul 10. Tech Vasc Interv Radiol. 2025. PMID: 40784682 Review.
-
Applications of percutaneous mechanical thrombectomy in transjugular intrahepatic portosystemic shunt and portal vein thrombosis.Tech Vasc Interv Radiol. 2003 Mar;6(1):59-69. doi: 10.1053/tvir.2003.36433. Tech Vasc Interv Radiol. 2003. PMID: 12772131 Review.
Cited by
-
Management of acute non-cirrhotic and non-malignant portal vein thrombosis: a systematic review.World J Surg. 2011 Nov;35(11):2510-20. doi: 10.1007/s00268-011-1198-0. World J Surg. 2011. PMID: 21882035
-
Catheter-directed thrombolysis through the operatively recanalized umbilical vein for acute extensive portal vein thrombosis: report of a case.Clin J Gastroenterol. 2014 Aug;7(4):376-80. doi: 10.1007/s12328-014-0510-6. Epub 2014 Jul 8. Clin J Gastroenterol. 2014. PMID: 26185890
-
Porto-spleno-mesenteric venous thrombosis after elective splenectomy: a retrospective cohort study.Front Immunol. 2023 Oct 20;14:1216283. doi: 10.3389/fimmu.2023.1216283. eCollection 2023. Front Immunol. 2023. PMID: 37928557 Free PMC article.
-
Initial transcatheter thrombolysis for acute superior mesenteric venous thrombosis.World J Gastroenterol. 2014 May 14;20(18):5483-92. doi: 10.3748/wjg.v20.i18.5483. World J Gastroenterol. 2014. PMID: 24833878 Free PMC article.
-
Mesenteric venous thrombosis in a young adult: A case report and review of the literature.World J Radiol. 2024 Oct 28;16(10):569-578. doi: 10.4329/wjr.v16.i10.569. World J Radiol. 2024. PMID: 39494142 Free PMC article.
References
-
- Sobhonslidsuk A, Reddy KR. Portal vein thrombosis: a concise review. Am J Gastroenterol. 2002;97:535–541. - PubMed
-
- Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345:1683–1688. - PubMed
-
- Brink JS, Brown AK, Palmer BA, Moir C, Rodeberg DR. Portal vein thrombosis after laparoscopy-assisted splenectomy and cholecystectomy. J Pediatr Surg. 2003;38:644–647. - PubMed
-
- Hassn AM, Al-Fallouji MA, Ouf TI, Saad R. Portal vein thrombosis following splenectomy. Br J Surg. 2000;87:362–373. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
