

Distribution and seasonality of rhinovirus and other respiratory viruses in a cross-section of asthmatic children in Trinidad, West Indies
- PMID: 19555507
- PMCID: PMC2717562
- DOI: 10.1186/1824-7288-35-16
Distribution and seasonality of rhinovirus and other respiratory viruses in a cross-section of asthmatic children in Trinidad, West Indies
Abstract
Background: Childhood asthma in the Caribbean is advancing in prevalence and morbidity. Though viral respiratory tract infections are reported triggers for exacerbations, information on these infections with asthma is sparse in Caribbean territories. We examined the distribution of respiratory viruses and their association with seasons in acute and stable asthmatic children in Trinidad.
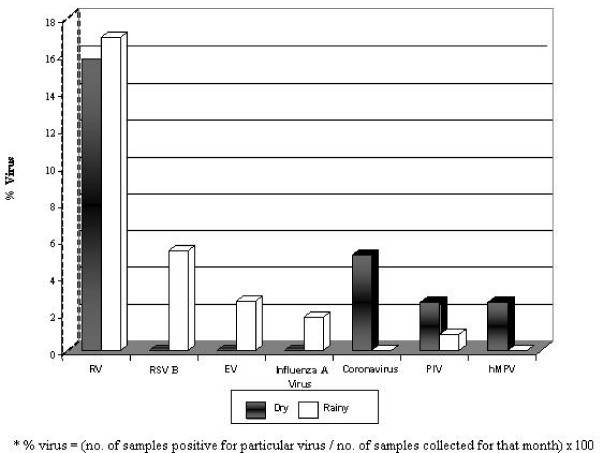
Methods: In a cross-sectional study of 70 wheezing children attending the emergency department for nebulisation and 80 stable control subjects (2 to 16 yr of age) in the asthma clinic, nasal specimens were collected during the dry (n = 38, January to May) and rainy (n = 112, June to December) seasons. A multitarget, sensitive, specific high-throughput Respiratory MultiCode assay tested for respiratory-virus sequences for eight distinct groups: human rhinovirus, respiratory syncytial virus, parainfluenza virus, influenza virus, metapneumovirus, adenovirus, coronavirus, and enterovirus.
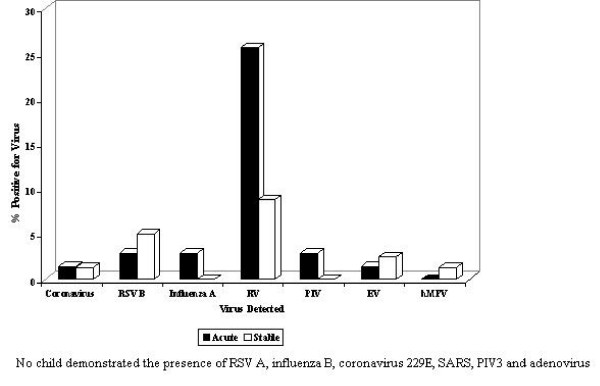
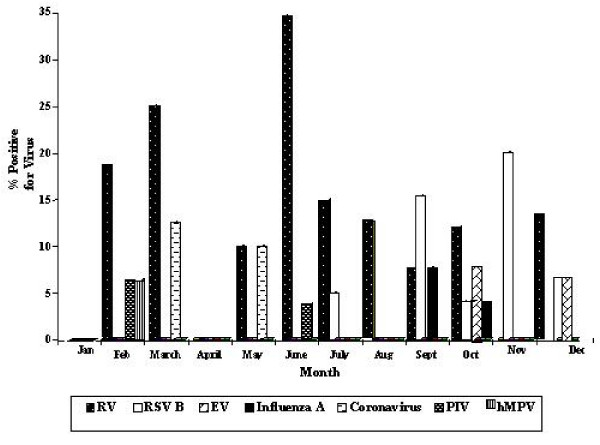
Results: Wheezing children had a higher [chi(2 )= 5.561, p = 0.018] prevalence of respiratory viruses compared with stabilized asthmatics (34.3% (24) versus (vs.) 17.5% (14)). Acute asthmatics were thrice as likely to be infected with a respiratory virus (OR = 2.5, 95% CI = 1.2 - 5.3). The predominant pathogens detected in acute versus stable asthmatics were the rhinovirus (RV) (n = 18, 25.7% vs. n = 7, 8.8%; p = 0.005), respiratory syncytial virus B (RSV B) (n = 2, 2.9% vs. n = 4, 5.0%), and enterovirus (n = 1, 1.4% vs. n = 2, 2.5%). Strong odds for rhinoviral infection were observed among nebulised children compared with stable asthmatics (p = 0.005, OR = 3.6, 95% CI = 1.4 - 9.3,). RV was prevalent throughout the year (Dry, n = 6, 15.8%; Rainy, n = 19, 17.0%) and without seasonal association [chi(2 )= 0.028, p = 0.867]. However it was the most frequently detected virus [Dry = 6/10, (60.0%); Rainy = 19/28, (67.9%)] in both seasons.
Conclusion: Emergent wheezing illnesses during childhood can be linked to infection with rhinovirus in Trinidad's tropical environment. Viral-induced exacerbations of asthma are independent of seasons in this tropical climate. Further clinical and virology investigations are recommended on the role of infections with the rhinovirus in Caribbean childhood wheeze.
Figures
References
-
- Heymann PW, Carper HT, Murphy DD, Platts-Mills TA, Patrie J, McLaughlin AP, Erwin EA, Shaker MS, Hellems M, Peerzada J, Hayden FG, Hatley TK, Chamberlain R. Viral infections in relation to age, atopy, and season of admission among children hospitalized for wheezing. J Allergy Clin Immunol. 2004;114:239–247. doi: 10.1016/j.jaci.2004.04.006. - DOI - PMC - PubMed
-
- Lemanske RF, Jr, Jackson DJ, Gangnon RE, Evans MD, Li Z, Shult PA, Kirk CJ, Reisdorf E, Roberg KA, Anderson EL, Carlson-Dakes KT, Adler KJ, Gilbertson-White S, Pappas TE, Dasilva DF, Tisler CJ, Gern JE. Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol. 2005;116:571–577. doi: 10.1016/j.jaci.2005.06.024. - DOI - PubMed
-
- Rakes GP, Arruda E, Ingram JM, Hoover GE, Zambrano JC, Hayden FG, Platts-Mills TA, Heymann PW. Rhinovirus and respiratory syncytial virus in wheezing children requiring emergency care. IgE and eosinophil analyses. Am J Respir Crit Care Med. 1999;159:785–790. - PubMed
LinkOut - more resources
Full Text Sources
