

A test of syndromic surveillance using a severe acute respiratory syndrome model
- PMID: 19555611
- PMCID: PMC7127470
- DOI: 10.1016/j.ajem.2008.03.020
A test of syndromic surveillance using a severe acute respiratory syndrome model
Abstract
Objectives: We describe a field simulation that was conducted using volunteers to assess the ability of 3 hospitals in a network to manage a large influx of patients with a potentially communicable disease. This drill provided the opportunity to evaluate the ability of the New York City Department of Health and Mental Hygiene's (NYC-DOHMH) emergency department chief complaint syndromic surveillance system to detect a cluster of patients with febrile respiratory illness.
Methods: The evaluation was a prospective simulation. The clinical picture was modeled on severe acute respiratory syndrome symptoms. Forty-four volunteers participated in the drill as mock patients.
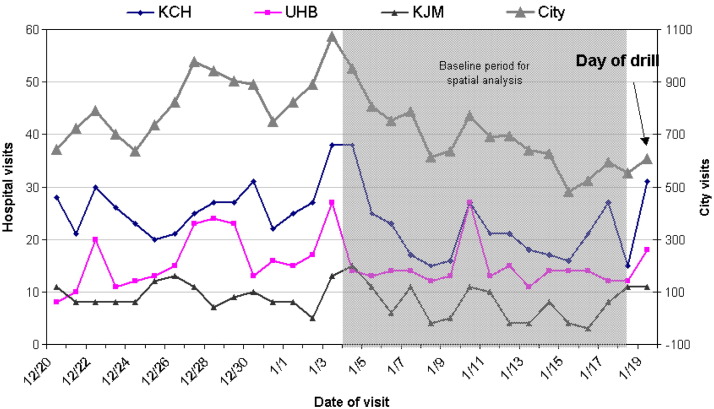
Results: Records from 42 patients (95%) were successfully transmitted to the NYC-DOHMH. The electronic chief complaint for 24 (57%) of these patients indicated febrile or respiratory illness. The drill did not generate a statistical signal in the NYC-DOHMH SaTScan analysis. The 42 drill patients were classified in 8 hierarchical categories based on chief complaints: sepsis (2), cold (3), diarrhea (2), respiratory (20), fever/flu (4), vomit (3), and other (8). The number of respiratory visits, while elevated on the day of the drill, did not appear particularly unusual when compared with the 14-day baseline period used for spatial analyses.
Conclusions: This drill with a cluster of patients with febrile respiratory illness failed to trigger a signal from the NYC-DOHMH emergency department chief complaint syndromic surveillance system. This highlighted several limitations and challenges to syndromic surveillance monitoring.
Figures
Similar articles
-
Field investigations of emergency department syndromic surveillance signals--New York City.MMWR Suppl. 2004 Sep 24;53:184-9. MMWR Suppl. 2004. PMID: 15717390
-
Should we be worried? Investigation of signals generated by an electronic syndromic surveillance system--Westchester County, New York.MMWR Suppl. 2004 Sep 24;53:190-5. MMWR Suppl. 2004. PMID: 15717391
-
Three years of emergency department gastrointestinal syndromic surveillance in New York City: what have we found?MMWR Suppl. 2005 Aug 26;54:175-80. MMWR Suppl. 2005. PMID: 16177711
-
Real-time syndrome surveillance in Ontario, Canada: the potential use of emergency departments and Telehealth.Eur J Emerg Med. 2004 Feb;11(1):3-11. doi: 10.1097/00063110-200402000-00002. Eur J Emerg Med. 2004. PMID: 15167186 Review.
-
Collateral damage: the unforeseen effects of emergency outbreak policies.Lancet Infect Dis. 2004 Nov;4(11):697-703. doi: 10.1016/S1473-3099(04)01176-4. Lancet Infect Dis. 2004. PMID: 15522682 Free PMC article. Review.
Cited by
-
The global pool of simulation exercise materials in health emergency preparedness and response: a scoping review with a health system perspective.BMJ Glob Health. 2019 Jul 29;4(4):e001687. doi: 10.1136/bmjgh-2019-001687. eCollection 2019. BMJ Glob Health. 2019. PMID: 31406594 Free PMC article.
References
-
- Buehler J.W., Hopkins R.S., Overhage J.M., Sosin D.M., Tong V. Framework for evaluating public health surveillance systems for early detection of outbreaks: recommendations from the CDC Working Group. MMWR Recomm Rep. 2004;53(RR-5):1–11. - PubMed
-
- Thacker S.B., Berkelman R.L. Public health surveillance in the United States. Epidemiol Rev. 1988;10:164–190. - PubMed
-
- Heffernan R., Mostashari F., Das D., Karpati A., Kulldorff M., Weiss D. Syndromic surveillance in public health practice, New York City. Emerg Infect Dis. 2004;10(5):858–864. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
