

Assessment of safety and feasibility of a new technical variant of gastropexy for percutaneous endoscopic gastrostomy: an experience with 435 cases
- PMID: 19558672
- PMCID: PMC2717113
- DOI: 10.1186/1471-230X-9-48
Assessment of safety and feasibility of a new technical variant of gastropexy for percutaneous endoscopic gastrostomy: an experience with 435 cases
Abstract
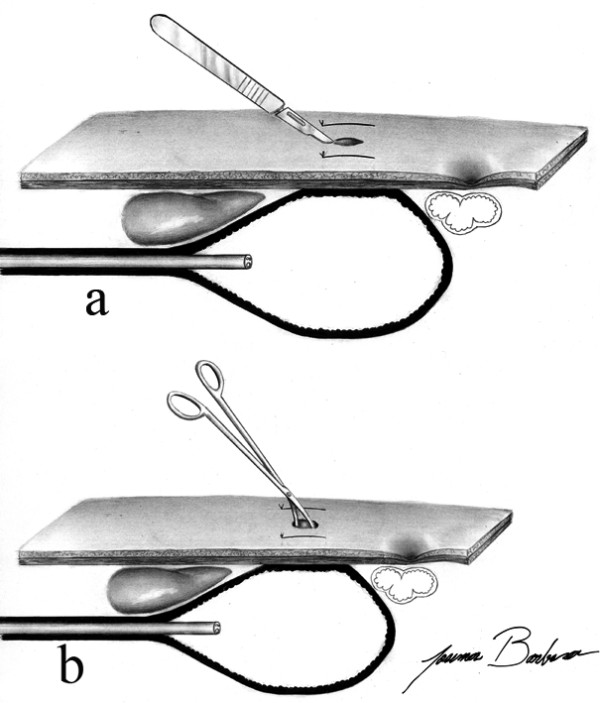
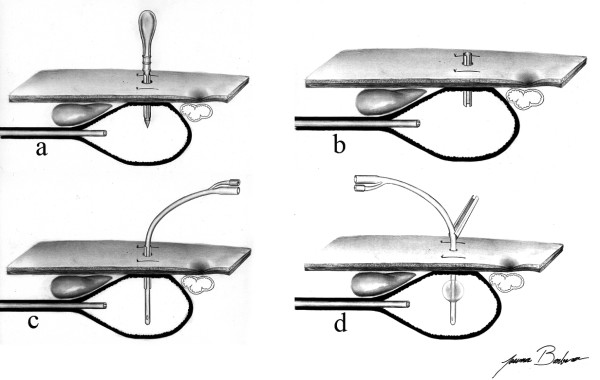
Background: Percutaneous Endoscopic Gastrostomy (PEG) performed through the Introducer Technique is associated with lower risk of surgical infection when compared to the Pull Technique. Its use is less widespread as the fixation of the stomach to the abdominal wall is a stage of the procedure that is difficult to be performed. We present a new technical variant of gastropexy which is fast and easy to be performed. The aim of this study was to evaluate the safety and feasibility of a new technical variant of gastropexy in patients submitted to gastrostomy performed through the Introducer Technique.
Methods: All the patients submitted to PEG through the Introducer Technique were evaluated using a new technical variant of gastropexy, which consists of two parallel stitches of trasfixation sutures involving the abdominal wall and the gastric wall, performed with a long curved needle. Prophylactic antibiotics were not used. Demographic aspects, initial diagnosis, indication, sedation doses, morbidity and surgical mortality were all analyzed.
Results: Four hundred and thirty-five consecutive PEGs performed between June 2004 and May 2007 were studied. Nearly all the cases consisted of patients presenting malignant neoplasia, 79.5% of which sited in the head and neck. The main indication of PEG was dysphagia, found in 346 patients (79.5%). There were 12 complications (2.8%) in 11 patients, from which only one patient had peristomal infection (0.2%). There was one death related to the procedure.
Conclusion: Gastropexy with the technical variant described here is easy to be performed and was feasible and safe in the present study. PEG performed by the Introducer Technique with this type of gastropexy was associated with low rates of wound infection even without the use of prophylactic antibiotics.
Figures


Similar articles
-
Complications in children with percutaneous endoscopic gastrostomy (PEG) placement.World J Pediatr. 2019 Feb;15(1):12-16. doi: 10.1007/s12519-018-0206-y. Epub 2018 Nov 19. World J Pediatr. 2019. PMID: 30456563 Review.
-
Peristomal infection in percutaneous endoscopic gastrostomy (PEG): a comparative study of two gastropexy techniques in a before-and-after design.Acta Gastroenterol Latinoam. 2011 Dec;41(4):296-301. Acta Gastroenterol Latinoam. 2011. PMID: 22292225
-
New "introducer" PEG-gastropexy with T fasteners: a pilot study.Arq Gastroenterol. 2011 Oct-Dec;48(4):231-5. doi: 10.1590/s0004-28032011000400003. Arq Gastroenterol. 2011. PMID: 22147126 Clinical Trial.
-
New introducer PEG gastropexy does not require prophylactic antibiotics: multicenter prospective randomized double-blind placebo-controlled study.Gastrointest Endosc. 2008 Apr;67(4):620-8. doi: 10.1016/j.gie.2007.10.044. Gastrointest Endosc. 2008. PMID: 18374024 Clinical Trial.
-
Abdominal wall metastasis following percutaneous endoscopic gastrostomy.Support Care Cancer. 1995 Sep;3(5):313-6. doi: 10.1007/BF00335308. Support Care Cancer. 1995. PMID: 8520878 Review.
Cited by
-
Surgery, fame, and misfortune: the life of Bronisław Kader.World J Surg. 2012 Aug;36(8):1998-2002. doi: 10.1007/s00268-012-1588-y. World J Surg. 2012. PMID: 22488328 Free PMC article.
-
Percutaneous Endoscopic Gastrostomy with Jejunal Extension Versus Direct Percutaneous Endoscopic Jejunostomy for Post-pyloric Feeding: A Dual-Center Retrospective Study.Dig Dis Sci. 2025 Jul 30. doi: 10.1007/s10620-025-09198-2. Online ahead of print. Dig Dis Sci. 2025. PMID: 40736945
-
Complications in children with percutaneous endoscopic gastrostomy (PEG) placement.World J Pediatr. 2019 Feb;15(1):12-16. doi: 10.1007/s12519-018-0206-y. Epub 2018 Nov 19. World J Pediatr. 2019. PMID: 30456563 Review.
-
Observation of the esophagus, pharynx and lingual root by gastrointestinal endoscopy with a percutaneous retrograde approach.World J Gastrointest Endosc. 2010 Aug 16;2(8):288-92. doi: 10.4253/wjge.v2.i8.288. World J Gastrointest Endosc. 2010. PMID: 21160628 Free PMC article.
-
Indications, complications and long-term follow-up of patients undergoing percutaneous endoscopic gastrostomy: A retrospective study.Wien Klin Wochenschr. 2012 Mar;124(5-6):148-53. doi: 10.1007/s00508-011-0082-0. Epub 2012 Mar 5. Wien Klin Wochenschr. 2012. PMID: 22382552
References
-
- Hashiba K. [Technic for opening a gastrostomy under endoscopic control and manipulation] Rev Paul Med. 1980;95(1–2):37–38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
