

White/black racial differences in risk of end-stage renal disease and death
- PMID: 19559170
- PMCID: PMC2749005
- DOI: 10.1016/j.amjmed.2008.11.021
White/black racial differences in risk of end-stage renal disease and death
Abstract
Background: End-stage renal disease disproportionately affects black persons, but it is unknown when in the course of chronic kidney disease racial differences arise. Understanding the natural history of racial differences in kidney disease may help guide efforts to reduce disparities.
Methods: We compared white/black differences in the risk of end-stage renal disease and death by level of estimated glomerular filtration rate (eGFR) at baseline in a national sample of 2,015,891 veterans between 2001 and 2005.
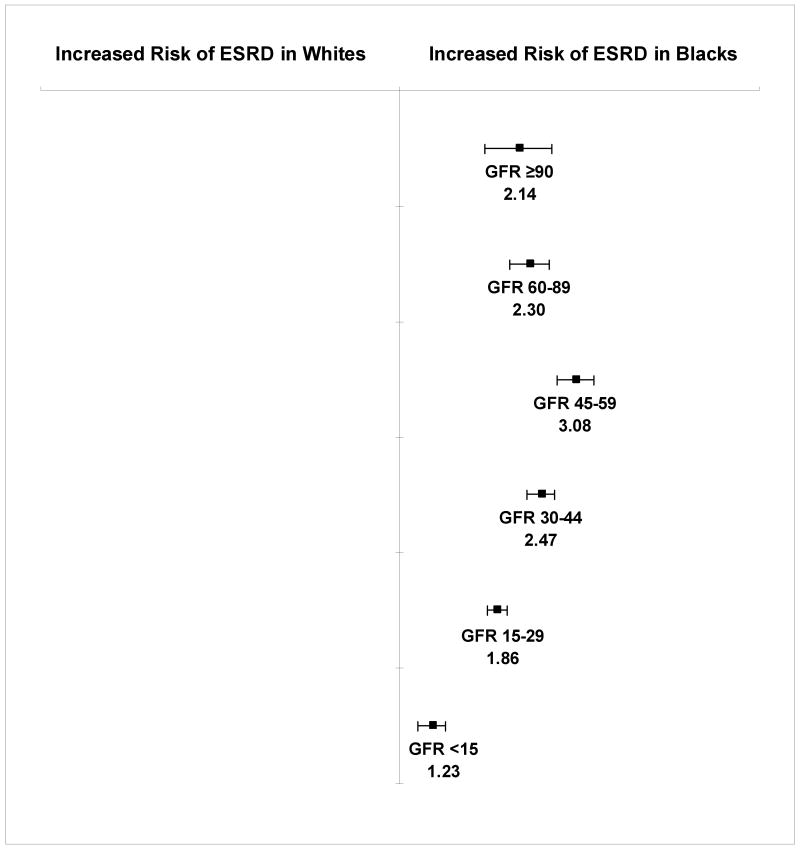
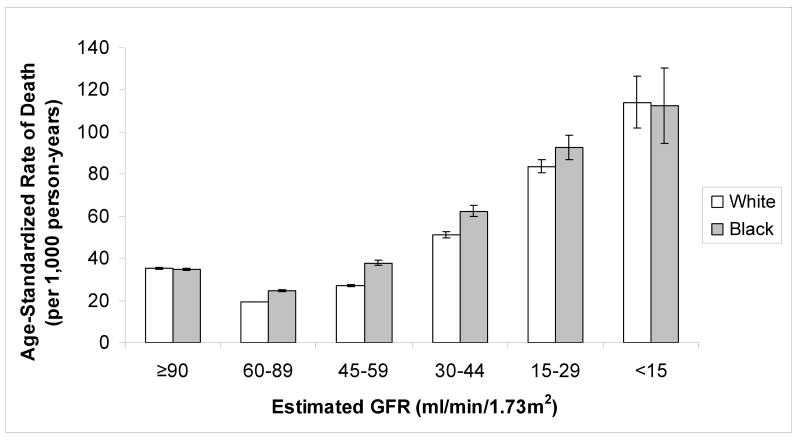
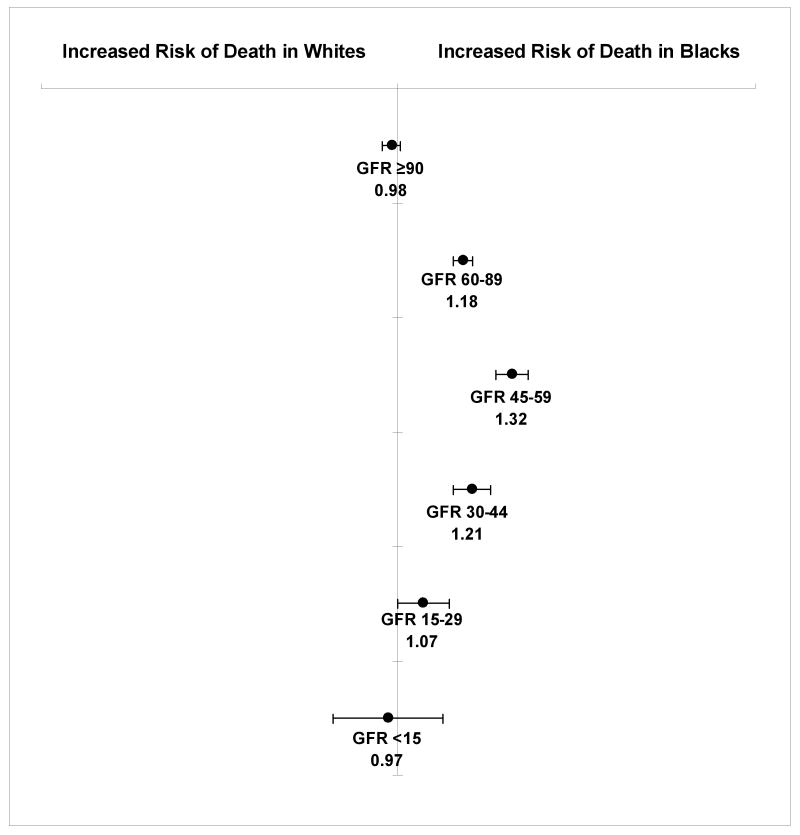
Results: Rates of end-stage renal disease among black patients exceeded those among white patients at all levels of baseline eGFR. The adjusted hazard ratios for end-stage renal disease associated with black versus white race for patients with an eGFR > or = 90, 60-89, 45-59, 30-44, 15-29, and <15 mL/min/1.73 m2, respectively, were 2.14 (95% confidence interval [CI], 1.72-2.65), 2.30 (95% CI, 2.02-2.61), 3.08 (95% CI, 2.74-3.46), 2.47 (95% CI, 2.26-2.70), 1.86 (95% CI, 1.75-1.98), and 1.23 (95% CI, 1.12-1.34). We observed a similar pattern for mortality, with equal or higher rates of death among black persons at all levels of eGFR. The highest risk of mortality associated with black race also was observed among those with an eGFR 45-59 mL/min/1.73 m2 (hazard ratio 1.32, 95% CI, 1.27-1.36).
Conclusion: Racial differences in the risk of end-stage renal disease appear early in the course of kidney disease and are not explained by a survival advantage among blacks. Efforts to identify and slow progression of chronic kidney disease at earlier stages may be needed to reduce racial disparities.
Conflict of interest statement
Figures
Comment in
-
Influence of Hispanic Ethnicity and Diabetic End-stage Renal Disease.Am J Med. 2010 Mar;123(3):e19; author reply e21. doi: 10.1016/j.amjmed.2009.08.025. Am J Med. 2010. PMID: 20193814 No abstract available.
References
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, et al. Chronic kidney disease as a global public health problem: Approaches and initiatives - a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007 Jun 13; - PubMed
-
- Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003 Jul 15;139(2):137–47. - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, et al. Prevalence of chronic kidney disease in the United States. Jama. 2007 Nov 7;298(17):2038–47. - PubMed
-
- United States Renal Data System 2006 Annual Data Report. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
