

Confocal laser endomicroscopy in Barrett's esophagus and endoscopically inapparent Barrett's neoplasia: a prospective, randomized, double-blind, controlled, crossover trial
- PMID: 19559419
- PMCID: PMC2755622
- DOI: 10.1016/j.gie.2009.02.009
Confocal laser endomicroscopy in Barrett's esophagus and endoscopically inapparent Barrett's neoplasia: a prospective, randomized, double-blind, controlled, crossover trial
Abstract
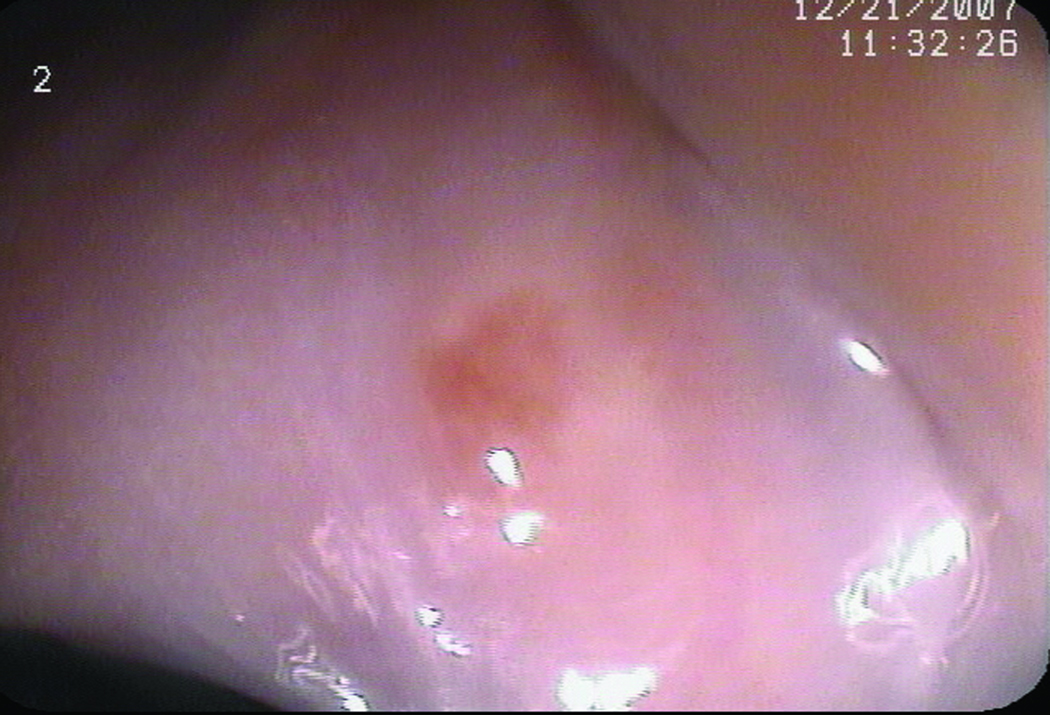
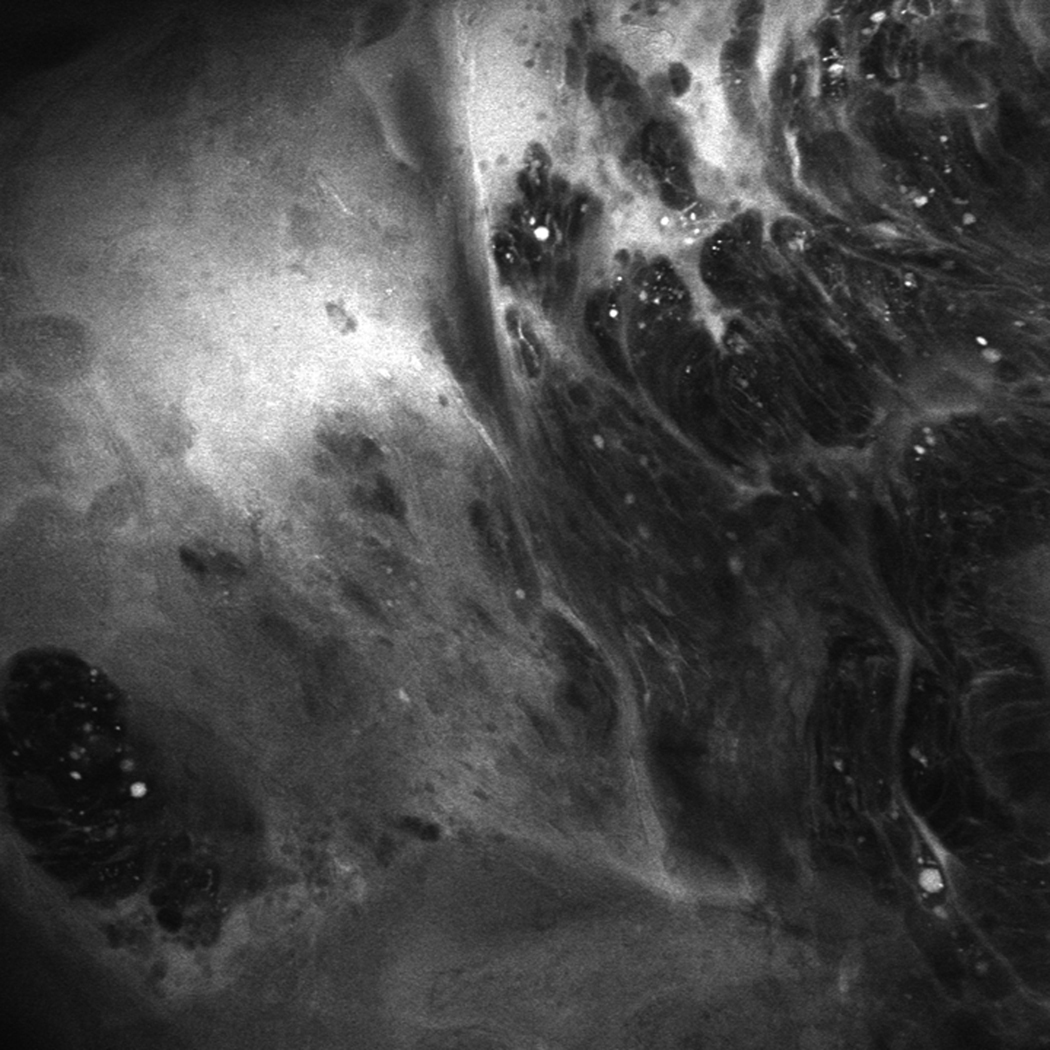
Background: The detection of high-grade dysplasia and cancer in Barrett's esophagus (BE) can be challenging. Confocal laser endomicroscopy (CLE) allows in vivo visualization of mucosal histology during endoscopy.
Objective: To determine whether CLE with optical biopsy and targeted mucosal biopsy improves the diagnostic yield of endoscopically inapparent, BE-associated neoplasia compared to standard endoscopy with a 4-quadrant, random biopsy protocol.
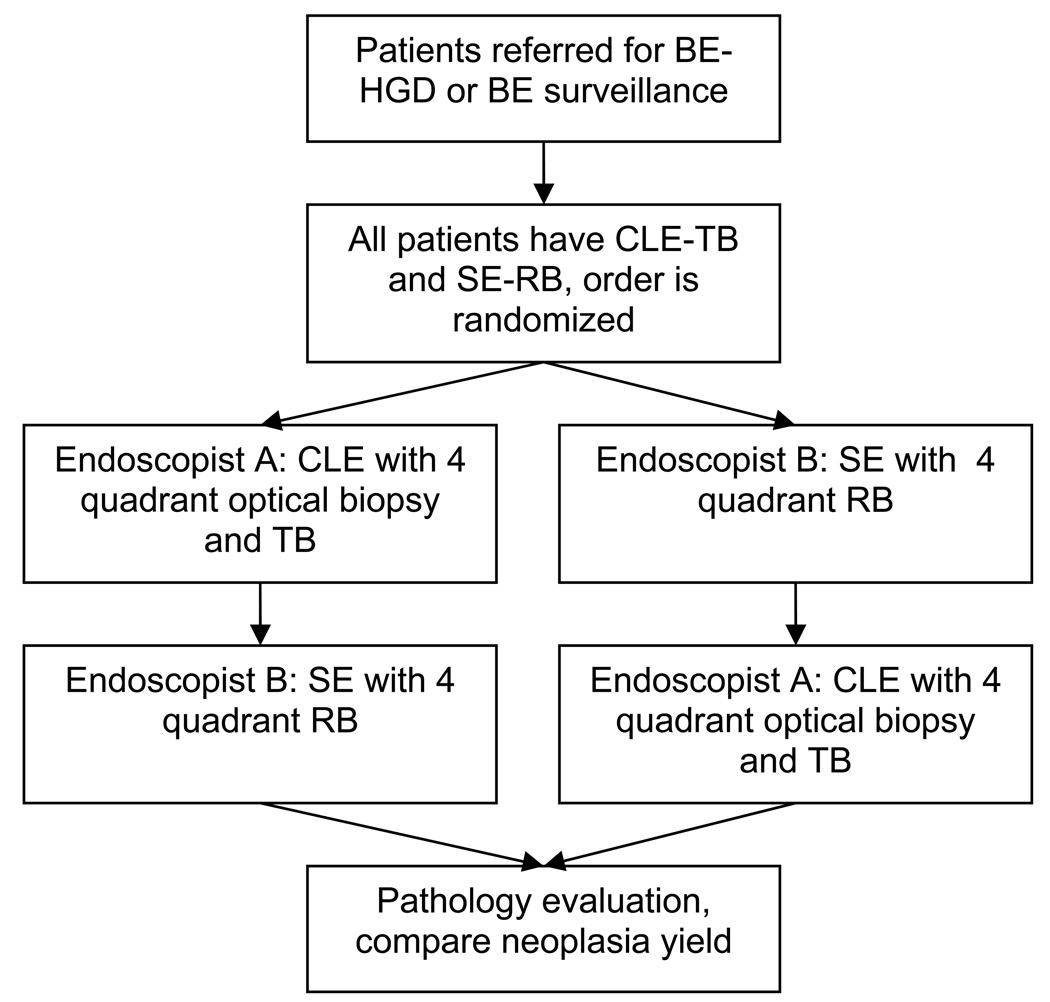
Design: Prospective, double-blind, randomized, crossover study.
Setting: Single, tertiary-care academic center.
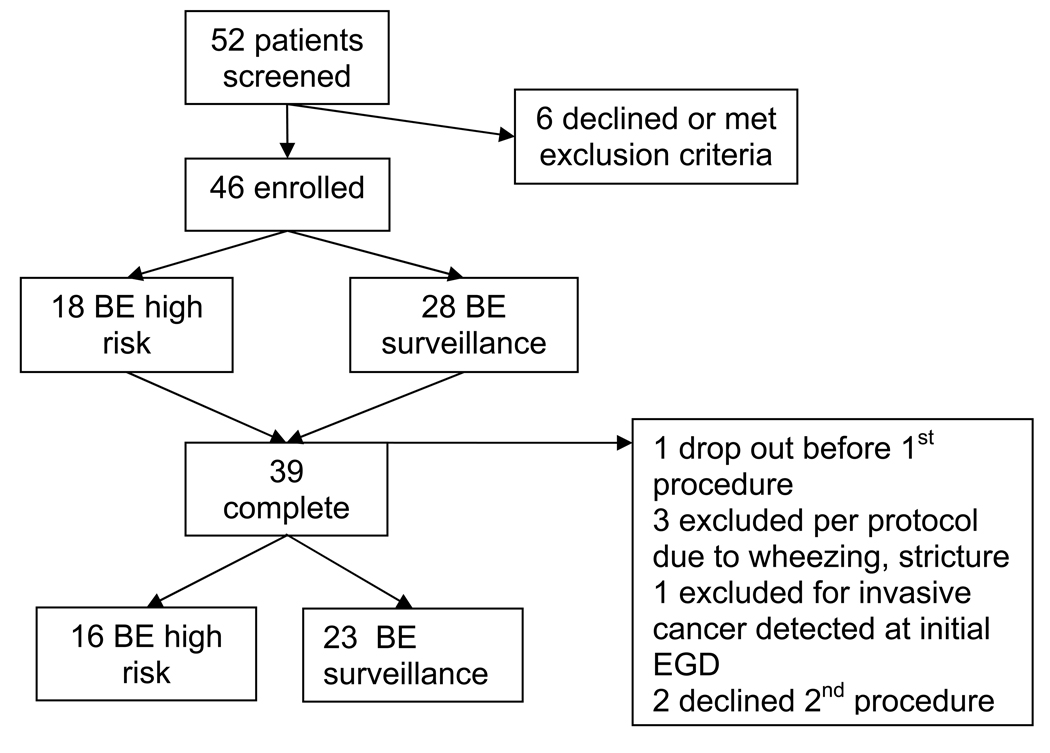
Patients: This study involved patients with BE undergoing routine surveillance or referred for treatment of nonlocalized, endoscopically inapparent, BE-associated neoplasia.
Intervention: All participants underwent both a confocal endomicroscopy with a targeted biopsy procedure and standard endoscopy with a 4-quadrant biopsy procedure in a randomized order.
Main outcome measurements: Increase in diagnostic yield for neoplasia, reduction in mucosal biopsy number, final pathologic diagnosis.
Results: CLE with targeted biopsy almost doubled the diagnostic yield for neoplasia and was equivalent to the standard protocol for the final diagnosis of neoplasia. Two thirds of patients in the surveillance group did not need any mucosal biopsies at all.
Limitation: Single-center study.
Conclusion: CLE with targeted biopsy significantly improves the diagnostic yield for endoscopically inapparent BE neoplasia compared to a standard endoscopy with a random-biopsy protocol. CLE with targeted biopsy also greatly reduces the number of biopsies needed per patient and allows some patients without neoplasia to completely forgo mucosal biopsy.
Trial registration: ClinicalTrials.gov NCT00487695.
Figures

Comment in
-
To perform a biopsy or not to perform a biopsy? Does confocal endomicroscopy provide the answer for surveillance in Barrett's esophagus?Gastrointest Endosc. 2009 Oct;70(4):655-7. doi: 10.1016/j.gie.2009.04.047. Gastrointest Endosc. 2009. PMID: 19788981 No abstract available.
References
-
- Falk GW. Barrett's esophagus. Gastroenterology. 2002;122:1569–1591. - PubMed
-
- Hirota WK, Zuckerman MJ, Adler DG, et al. ASGE guideline: the role of endoscopy in the surveillance of premalignant conditions of the upper GI tract. Gastrointest Endosc. 2006;63:570–580. - PubMed
-
- Wang KK, Sampliner RE. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barrett's esophagus. Am J Gastroenterol. 2008;103:788–797. - PubMed
-
- Reid BJ, Blount PL, Feng Z, et al. Optimizing endoscopic biopsy detection of early cancers in Barrett's high-grade dysplasia. Am J Gastroenterol. 2000;95:3089–3096. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
