

Acupuncture mobilizes the brain's default mode and its anti-correlated network in healthy subjects
- PMID: 19559684
- PMCID: PMC3742122
- DOI: 10.1016/j.brainres.2009.06.061
Acupuncture mobilizes the brain's default mode and its anti-correlated network in healthy subjects
Erratum in
- Brain Res. 2010 Jan 13;1308:185
Abstract
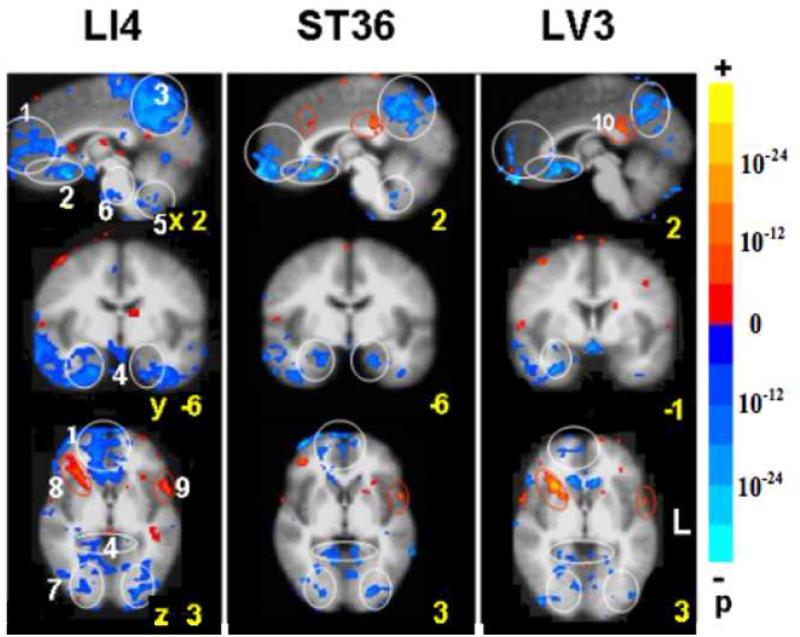
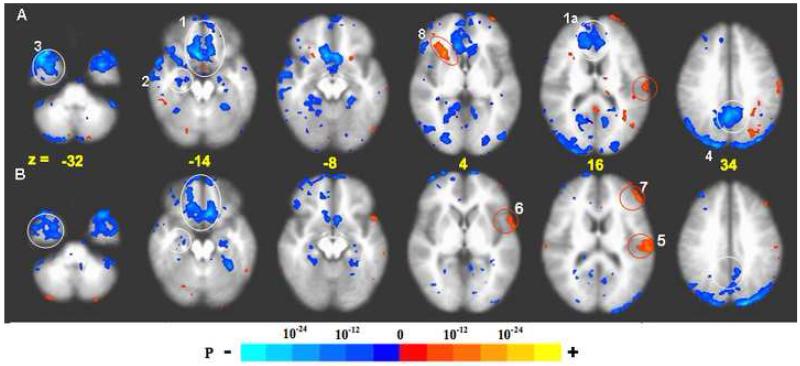
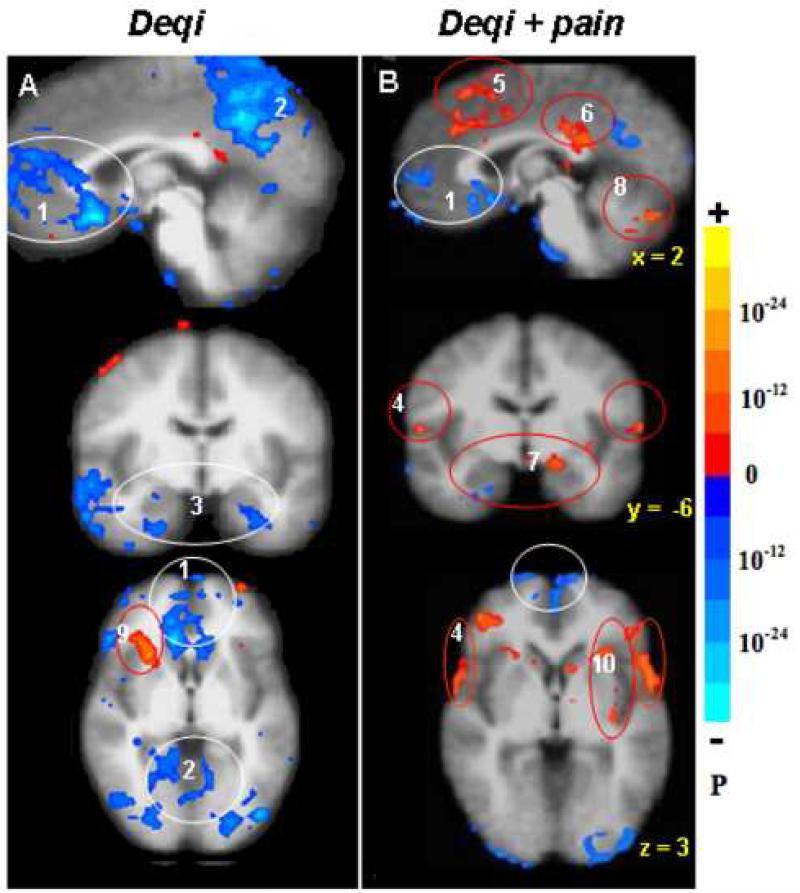
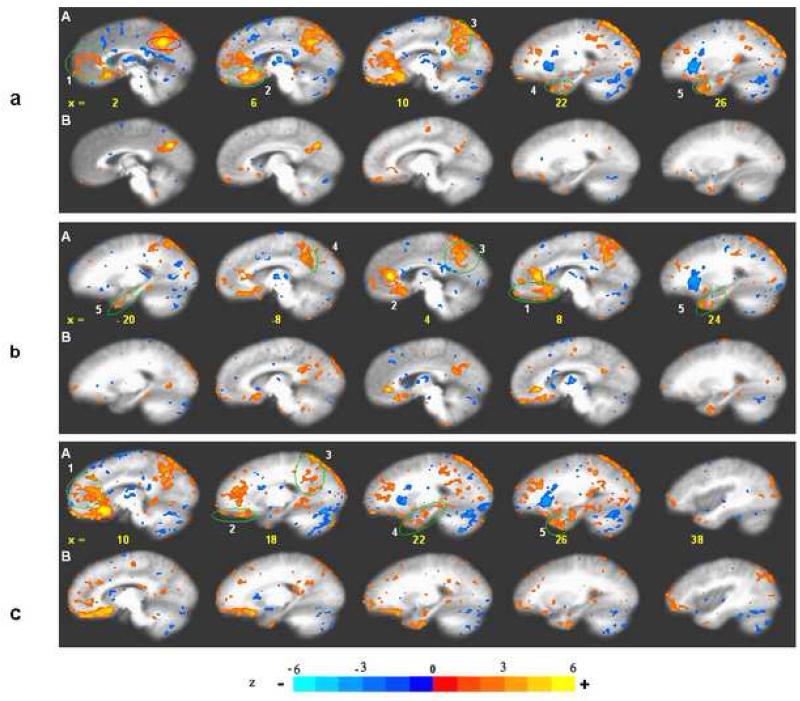
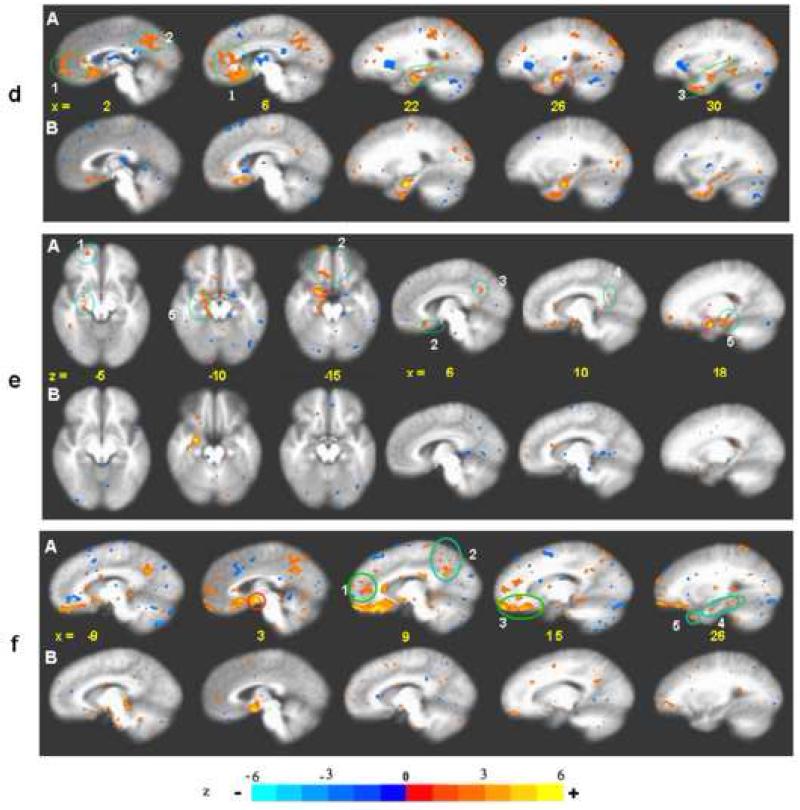
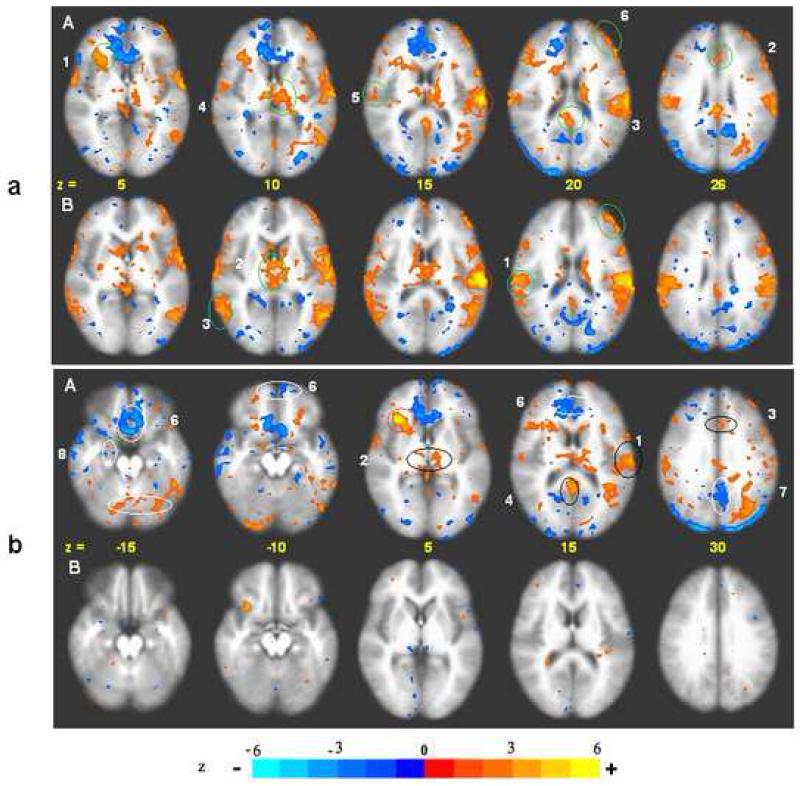
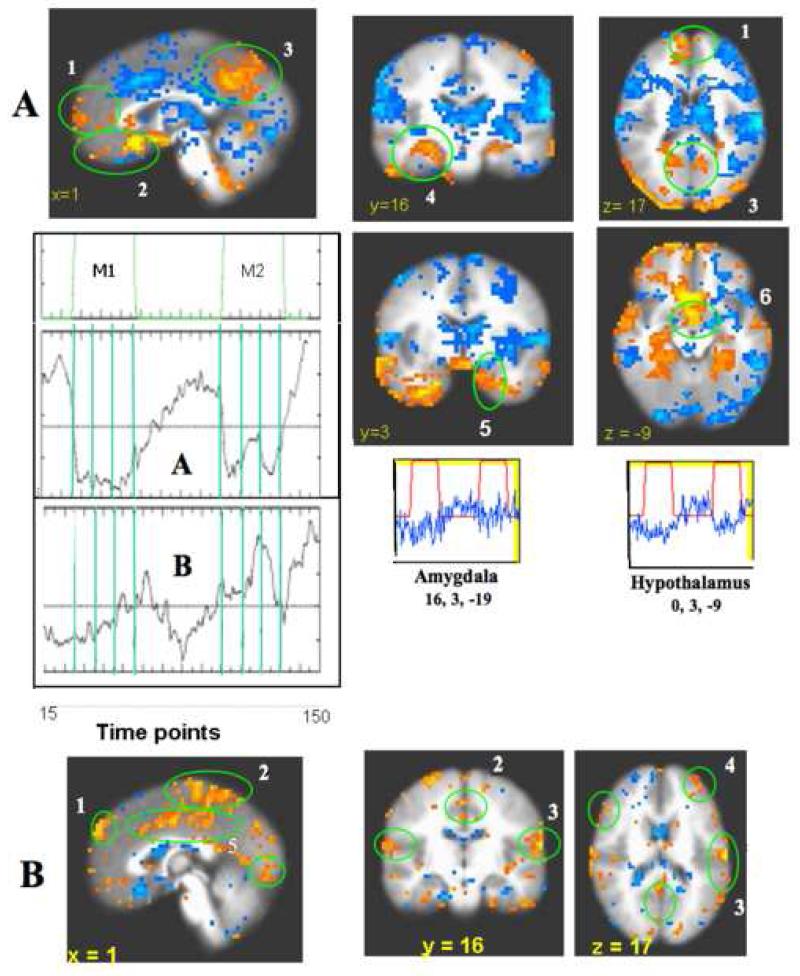
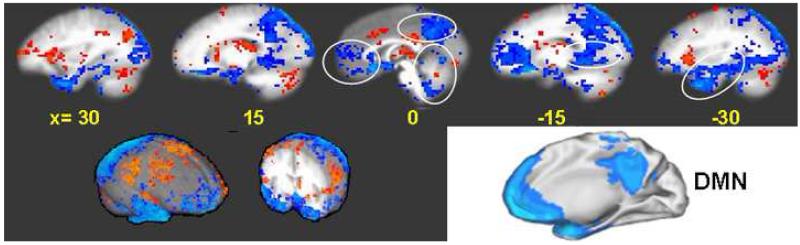
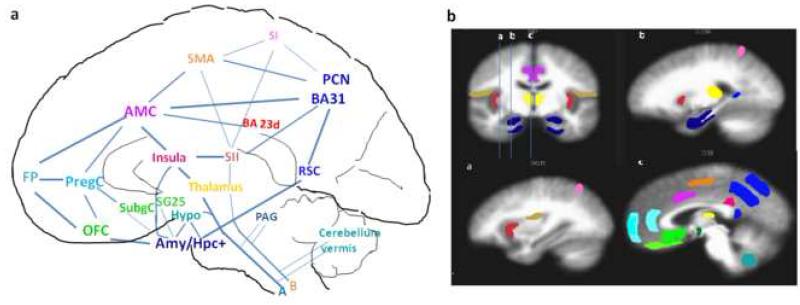
Previous work has shown that acupuncture stimulation evokes deactivation of a limbic-paralimbic-neocortical network (LPNN) as well as activation of somatosensory brain regions. This study explores the activity and functional connectivity of these regions during acupuncture vs. tactile stimulation and vs. acupuncture associated with inadvertent sharp pain. Acupuncture during 201 scans and tactile stimulation during 74 scans for comparison at acupoints LI4, ST36 and LV3 was monitored with fMRI and psychophysical response in 48 healthy subjects. Clusters of deactivated regions in the medial prefrontal, medial parietal and medial temporal lobes as well as activated regions in the sensorimotor and a few paralimbic structures can be identified during acupuncture by general linear model analysis and seed-based cross correlation analysis. Importantly, these clusters showed virtual identity with the default mode network and the anti-correlated task-positive network in response to stimulation. In addition, the amygdala and hypothalamus, structures not routinely reported in the default mode literature, were frequently involved in acupuncture. When acupuncture induced sharp pain, the deactivation was attenuated or became activated instead. Tactile stimulation induced greater activation of the somatosensory regions but less extensive deactivation of the LPNN. These results indicate that the deactivation of the LPNN during acupuncture cannot be completely explained by the demand of attention that is commonly proposed in the default mode literature. Our results suggest that acupuncture mobilizes the anti-correlated functional networks of the brain to mediate its actions, and that the effect is dependent on the psychophysical response.
Figures

References
-
- Apkarian AV, Bushnell MC, Treede Rolf-Detlef, Zubieta Jon-Kar. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9:463–484. - PubMed
-
- Beckmann CF, Smith SM. Probabilistic independent component analysis for functional magnetic resonance imaging. IEEE Trans Med Imaging. 2004;23(2):137–52. - PubMed
-
- Beckmann CF, Smith SM. Tensorial extensions of independent component analysis for multisubject FMRI analysis. Neuroimage. 2005;25(1):294–311. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
