

Arrhythmogenic right ventricular cardiomyopathy/dysplasia clinical presentation and diagnostic evaluation: results from the North American Multidisciplinary Study
- PMID: 19560088
- PMCID: PMC2735220
- DOI: 10.1016/j.hrthm.2009.03.013
Arrhythmogenic right ventricular cardiomyopathy/dysplasia clinical presentation and diagnostic evaluation: results from the North American Multidisciplinary Study
Abstract
Background: Prior reports on patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) focused on individuals with advanced forms of the disease. Data on the diagnostic performance of various testing modalities in newly identified individuals suspected of having ARVC/D are limited.
Objective: The purpose of the Multidisciplinary Study of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia was to study the clinical characteristics and diagnostic evaluation of a large group of patients newly identified with ARVC/D.
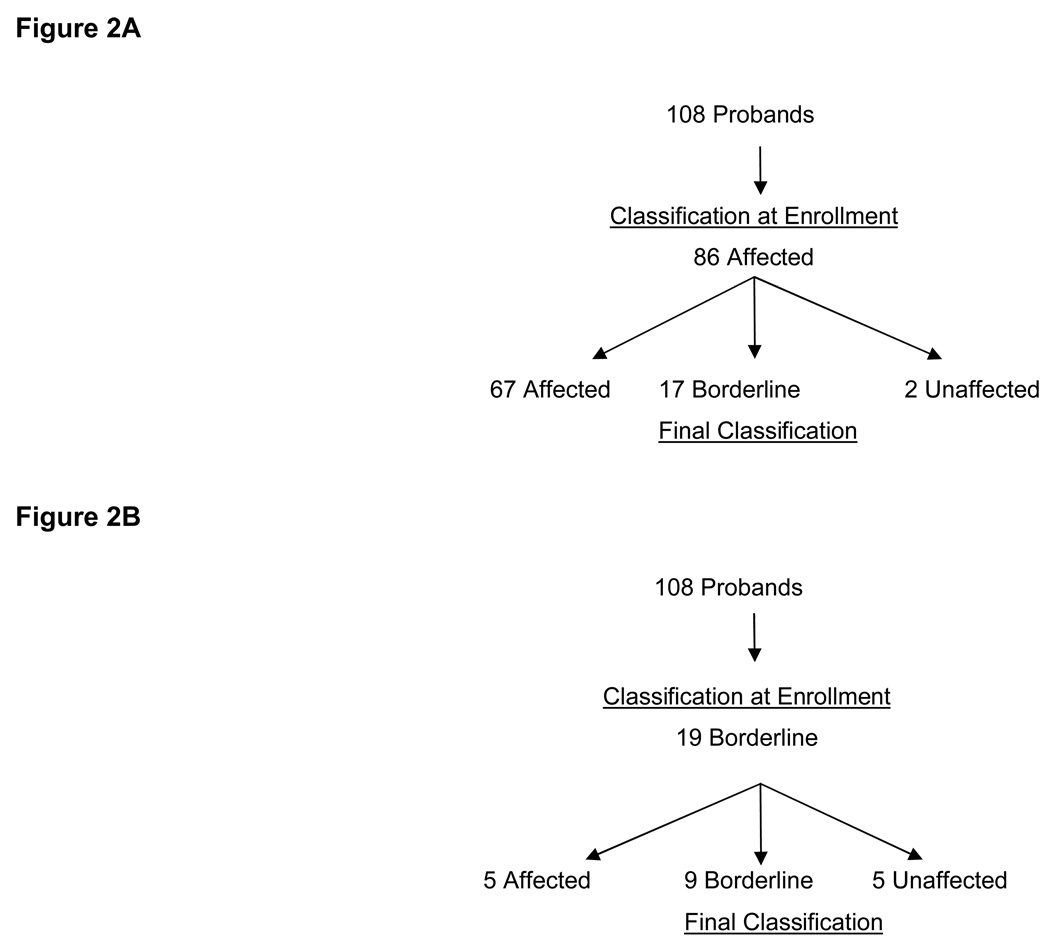
Methods: A total of 108 newly diagnosed patients with suspected ARVC/D were prospectively enrolled in the United States and Canada. The patients underwent noninvasive and invasive tests using standardized protocols that initially were interpreted by the enrolling center and adjudicated by blind analysis in six core laboratories. Patients were followed for a mean of 27 +/- 16 months (range 0.2-63 months).
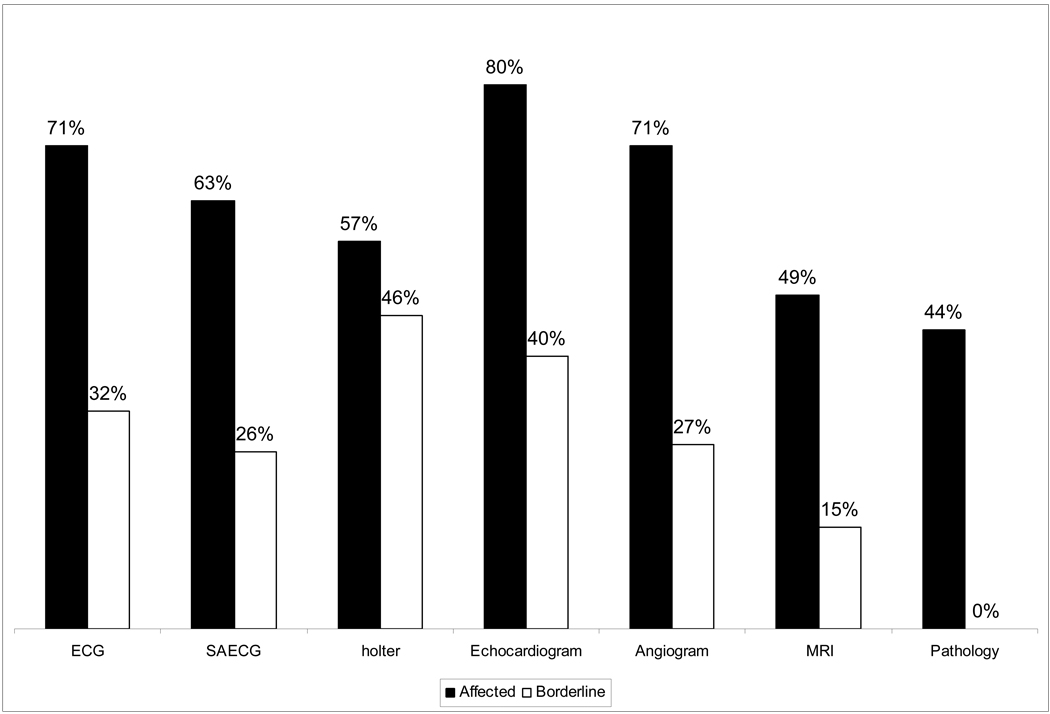
Results: The clinical profile of these newly diagnosed patients differs from the profile of reported patients with more advanced disease. There was considerable difference in the initial and final classification of the presence of ARVC/D after the diagnostic tests were evaluated by the core laboratories. Final clinical diagnosis was 73 affected, 28 borderline, and 7 unaffected. Individual tests agreed with the final diagnosis in 50% to 70% of the 73 patients with a final classification of affected.
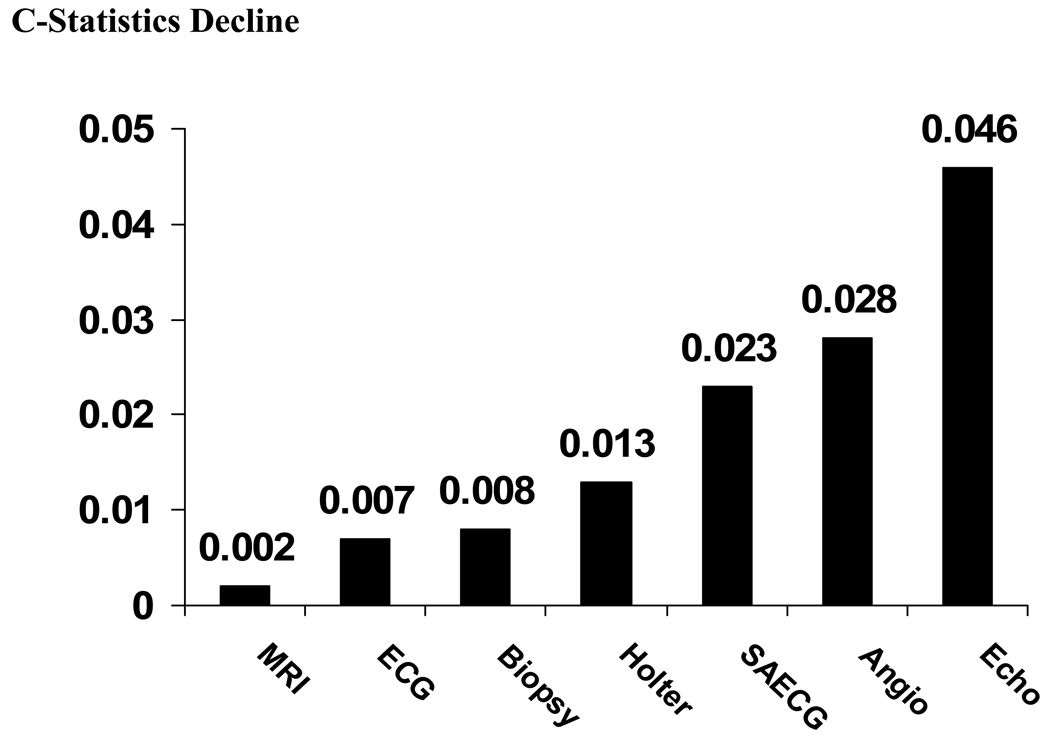
Conclusion: The clinical profile of 108 newly diagnosed probands with suspected ARVC/D indicates that a combination of diagnostic tests is needed to evaluate the presence of right ventricular structural, functional, and electrical abnormalities. Echocardiography, right ventricular angiography, signal-averaged ECG, and Holter monitoring provide optimal clinical evaluation of patients suspected of ARVC/D.
Conflict of interest statement
No conflict of interest
Figures

Comment in
-
Arrhythmogenic right ventricular cardiomyopathy/dysplasia.Heart Rhythm. 2009 Nov;6(11):e1; author reply e1-2. doi: 10.1016/j.hrthm.2009.09.002. Epub 2009 Sep 3. Heart Rhythm. 2009. PMID: 19879529 No abstract available.
References
-
- Marcus FI, Fontaine G. Arrhythmogenic right ventricular dysplasia/cardiomyopathy, a review. Pacing Clin Electrophysiol. 1995;18:1298–1314. - PubMed
-
- Kies P, Bootsma M, Bax J, et al. Arrhythmogenic right ventricular dysplasia/cardiomyopathy: Screening, diagnosis, and treatment. Heart Rhythm. 2006;3:225–234. - PubMed
-
- Sen-Chowdhry S, Lowe MD, Sporton SC, et al. Arrhythmogenic right ventricular cardiomyopathy: clinical presentation, diagnosis, and management. Am. J.Medicine. 2004;117:685–695. - PubMed
-
- Thiene G, Nava A, Corrado D, et al. Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med. 1988;318:129–133. - PubMed
-
- Maron BJ. Cardiovascular risks to young persons on the athletic field. Ann Int Med. 1998;129:379–386. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
