

Radiosurgery for spinal malignant tumors
- PMID: 19562022
- PMCID: PMC2696242
- DOI: 10.3238/arztebl.2009.0106
Radiosurgery for spinal malignant tumors
Abstract
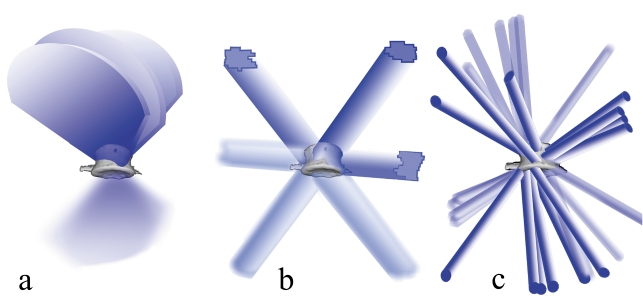
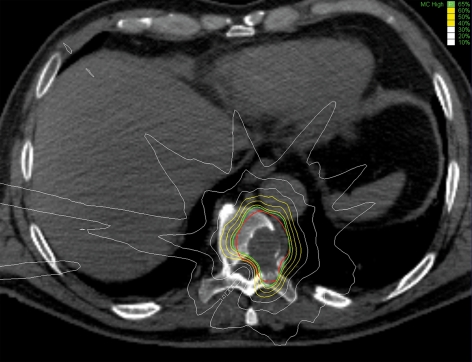
Background: Radiosurgery is a special treatment method that employs highly focused radiation to destroy tumors with high precision in a single session. A broad base of scientific evidence already exists for the radiosurgical treatment of brain metastases. Recent advances in medical technology now allow radiosurgery to be extended to the spine as well.
Methods: Selective literature review based on a PubMed search using the search terms stereotaxis, radiosurgery, stereotactic radiotherapy, accuracy, quality assurance, spine, spine metastasis, pain, Novalis, CyberKnife, Synergy, and robotics. We also present and analyze our own data as an illustration of the application of spinal radiosurgery.
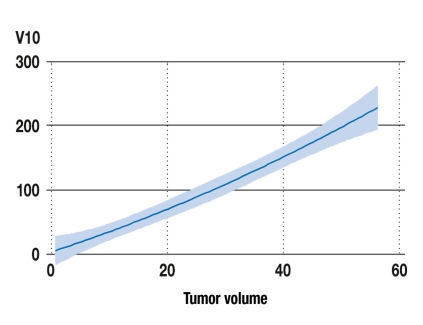
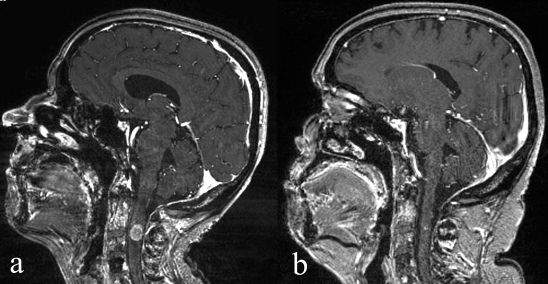
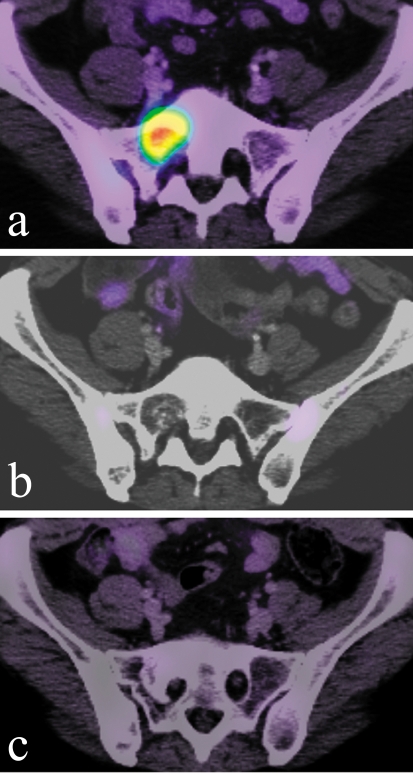
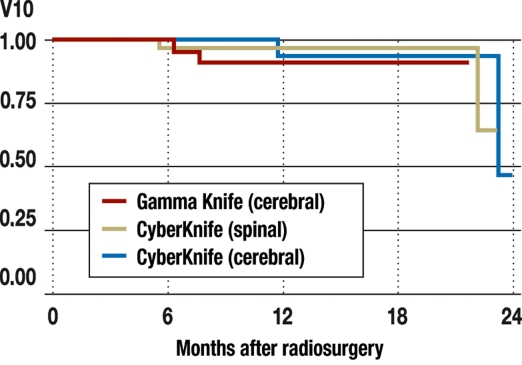
Results: The literature search identified 20 scientific original publications and one recent review. The data indicate that, within the specific constraints of the method, radiosurgery can arrest the growth of up to 96% of spinal metastases. Durable pain relief can be achieved in patients with tumor-associated pain syndromes. The morbidity of spinal radiosurgery is low, with a less than 1% risk of myelopathy.
Conclusions: Spinal radiosurgery is an independent, essentially noninvasive method of treatment. Different types of radiosurgical treatment apparatus are available. For properly selected patients, radiosurgery offers a good chance of therapeutic success with relatively rare complications.
Keywords: cancer treatment; medical technology; quality of life; radiation therapy; surgery.
Figures
Similar articles
-
Regarding: Rosenthal DI, Glatstein E. "We've Got a Treatment, but What's the Disease?" The Oncologist 1996;1.Oncologist. 1997;2(1):59-61. Oncologist. 1997. PMID: 10388030
-
CyberKnife radiosurgery for malignant spinal tumors: characterization of well-suited patients.Spine (Phila Pa 1976). 2008 Dec 15;33(26):2929-34. doi: 10.1097/BRS.0b013e31818c680a. Spine (Phila Pa 1976). 2008. PMID: 19092627
-
Spinal radiosurgery: technology and clinical outcomes.Neurosurg Rev. 2009 Jan;32(1):1-12; discussion 12-3. doi: 10.1007/s10143-008-0167-z. Epub 2008 Sep 24. Neurosurg Rev. 2009. PMID: 18813965 Review.
-
Image-guided and intensity-modulated radiosurgery for patients with spinal metastasis.Cancer. 2003 Apr 15;97(8):2013-8. doi: 10.1002/cncr.11296. Cancer. 2003. PMID: 12673732
-
Cyberknife radiosurgery for metastatic spine tumors.Neurosurg Clin N Am. 2004 Oct;15(4):491-501. doi: 10.1016/j.nec.2004.04.013. Neurosurg Clin N Am. 2004. PMID: 15450884 Review.
Cited by
-
Expertise is crucial.Dtsch Arztebl Int. 2009 May;106(19):340; author reply 340. doi: 10.3238/arztebl.2009.0340a. Epub 2009 May 8. Dtsch Arztebl Int. 2009. PMID: 19547735 Free PMC article. No abstract available.
-
Spinal radiosurgery--efficacy and safety after prior conventional radiotherapy.Radiat Oncol. 2011 Dec 16;6:173. doi: 10.1186/1748-717X-6-173. Radiat Oncol. 2011. PMID: 22177519 Free PMC article.
-
Evaluation of efficacy and safety of robotic stereotactic body radiosurgery and hypofractionated stereotactic radiotherapy for vertebral metastases.Contemp Oncol (Pozn). 2015;19(4):327-32. doi: 10.5114/wo.2015.53371. Epub 2015 Aug 7. Contemp Oncol (Pozn). 2015. PMID: 26557782 Free PMC article.
-
Bone metastases in thyroid cancer.J Bone Oncol. 2020 Feb 19;21:100282. doi: 10.1016/j.jbo.2020.100282. eCollection 2020 Apr. J Bone Oncol. 2020. PMID: 32154098 Free PMC article. Review.
-
Management and outcome in adult intramedullary spinal cord tumours: a 20-year single institution experience.BMC Res Notes. 2014 Dec 15;7:908. doi: 10.1186/1756-0500-7-908. BMC Res Notes. 2014. PMID: 25495874 Free PMC article.
References
-
- Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951;102:316–319. - PubMed
-
- Sturm V, Kober B, Hover KH, et al. Stereotactic percutaneous single dose irradiation of brain metastases with a linear accelerator. Int J Radiat Oncol Biol Phys. 1987;13:279–282. - PubMed
-
- Barnett GH, Linskey ME, Adler JR, et al. Stereotactic radiosurgery—an organized neurosurgery-sanctioned definition. J Neurosurg. 2007;106:1–5. - PubMed
-
- Sahgal A, Larson DA, Chang EL. Stereotactic body radiosurgery for spinal metastases: a critical review. Int J Radiat Oncol Biol Phys. 2008;71:652–665. - PubMed
-
- Muacevic A, Wowra B, Siefert A, Tonn JC, Steiger HJ, Kreth FW. Microsurgery plus whole brain irradiation versus Gamma Knife surgery alone for treatment of single metastases to the brain: a randomized controlled multicentre phase III trial. J Neurooncol. 2008;87:299–307. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources