

Role of pathogenic oral flora in postoperative pneumonia following brain surgery
- PMID: 19563632
- PMCID: PMC2709628
- DOI: 10.1186/1471-2334-9-104
Role of pathogenic oral flora in postoperative pneumonia following brain surgery
Abstract
Background: Post-operative pulmonary infection often appears to result from aspiration of pathogens colonizing the oral cavity. It was hypothesized that impaired periodontal status and pathogenic oral bacteria significantly contribute to development of aspiration pneumonia following neurosurgical operations. Further, the prophylactic effects of a single dose preoperative cefazolin on the oral bacteria were investigated.
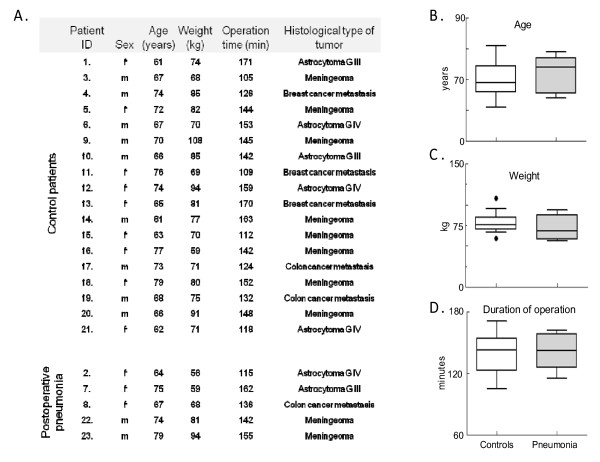
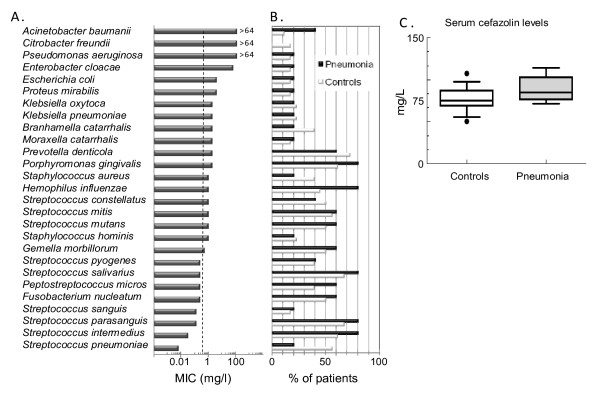
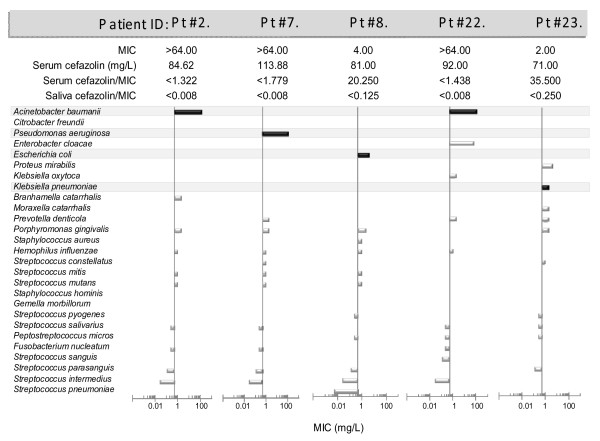
Methods: A matched cohort of 18 patients without postoperative lung complications was compared to 5 patients who developed pneumonia within 48 hours after brain surgery. Patients waiting for elective operation of a single brain tumor underwent dental examination and saliva collection before surgery. Bacteria from saliva cultures were isolated and periodontal disease was scored according to type and severity. Patients received 15 mg/kg cefazolin intravenously at the beginning of surgery. Serum, saliva and bronchial secretion were collected promptly after the operation. The minimal inhibitory concentrations of cefazolin regarding the isolated bacteria were determined. The actual antibiotic concentrations in serum, saliva and bronchial secretion were measured by capillary electrophoresis upon completion of surgery. Bacteria were isolated again from the sputum of postoperative pneumonia patients.
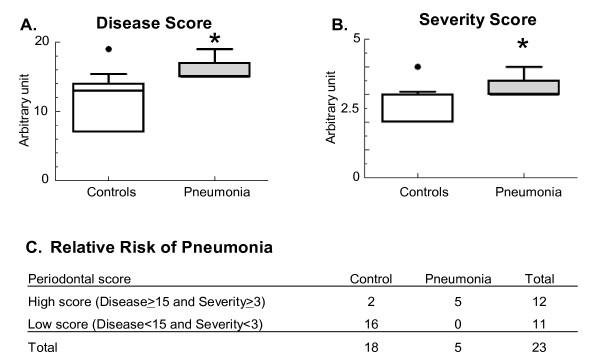
Results: The number and severity of coexisting periodontal diseases were significantly greater in patients with postoperative pneumonia in comparison to the control group (p = 0.031 and p = 0.002, respectively). The relative risk of developing postoperative pneumonia in high periodontal score patients was 3.5 greater than in patients who had low periodontal score (p < 0.0001). Cefazolin concentration in saliva and bronchial secretion remained below detectable levels in every patient.
Conclusion: Presence of multiple periodontal diseases and pathogenic bacteria in the saliva are important predisposing factors of postoperative aspiration pneumonia in patients after brain surgery. The low penetration rate of cefazolin into the saliva indicates that its prophylactic administration may not be sufficient to prevent postoperative aspiration pneumonia. Our study suggests that dental examination may be warranted in order to identify patients at high risk of developing postoperative respiratory infections.
Figures
References
-
- Hayes C, Sparrow D, Cohen M, Vokonas PS, Garcia RI. The association between alveolar bone loss and pulmonary function: the VA Dental Longitudinal Study. Ann Periodontol. 1998;3:257–261. - PubMed
-
- Scannapieco FA, Mylotte JM. Relationships between periodontal disease and bacterial pneumonia. J Periodontol. 1996;67:1114–1122. - PubMed
