

Identifying the etiology: a systematic approach using delayed-enhancement cardiovascular magnetic resonance
- PMID: 19564013
- PMCID: PMC2704908
- DOI: 10.1016/j.hfc.2009.02.009
Identifying the etiology: a systematic approach using delayed-enhancement cardiovascular magnetic resonance
Abstract
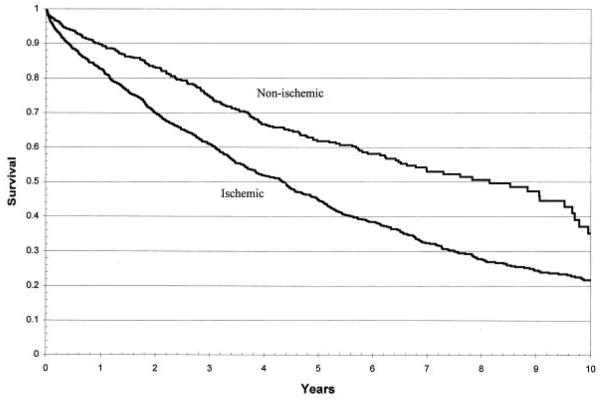
In patients who have heart failure, treatment and survival are directly related to the cause. Clinically, as a practical first step, patients are classified as having either ischemic or non-ischemic cardiomyopathy, a delineation usually based on the presence or absence of epicardial coronary artery disease. However, this approach does not account for patients with non-ischemic cardiomyopathy who also have coronary artery disease, which may be either incidental or partly contributing to myocardial dysfunction (mixed cardiomyopathy). By allowing direct assessment of the myocardium, delayed-enhancement cardiovascular magnetic resonance (DE-CMR) may aid in addressing these conundrums. This article explores the use of DE-CMR in identifying ischemic and non-ischemic myopathic processes and details a systematic approach to determine the cause of cardiomyopathy.
Figures
References
-
- Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O’Connell J, Olsen E, Thiene G, Goodwin J, Gyarfas I, Martin I, Nordet P. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation. 1996;93(5):841–842. - PubMed
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113(14):1807–1816. - PubMed
-
- Alderman EL, Fisher LD, Litwin P, Kaiser GC, Myers WO, Maynard C, Levine F, Schloss M. Results of coronary artery surgery in patients with poor left ventricular function (CASS) Circulation. 1983;68(4):785–795. - PubMed
-
- Felker GM, Shaw LK, O’Connor CM. A standardized definition of ischemic cardiomyopathy for use in clinical research. J Am Coll Cardiol. 2002;39(2):210–218. - PubMed
-
- Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P, Rouleau JL, Tendera M, Castaigne A, Roecker EB, Schultz MK, DeMets DL. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med. 2001;344(22):1651–1658. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
