

Dropout from outpatient mental health care in the United States
- PMID: 19564219
- PMCID: PMC2774713
- DOI: 10.1176/ps.2009.60.7.898
Dropout from outpatient mental health care in the United States
Abstract
Objective: Although mental health treatment dropout is common, patterns and predictors of dropout are poorly understood. This study explored patterns and predictors of mental health treatment dropout in a nationally representative sample.
Methods: Data were from the National Comorbidity Survey Replication, a nationally representative household survey. Respondents who had received mental health treatment in the 12 months before the interview (N=1,664) were asked about dropout, which was defined as quitting treatment before the provider wanted them to stop. Cross-tabulation and discrete-time survival analyses were used to identify predictors.
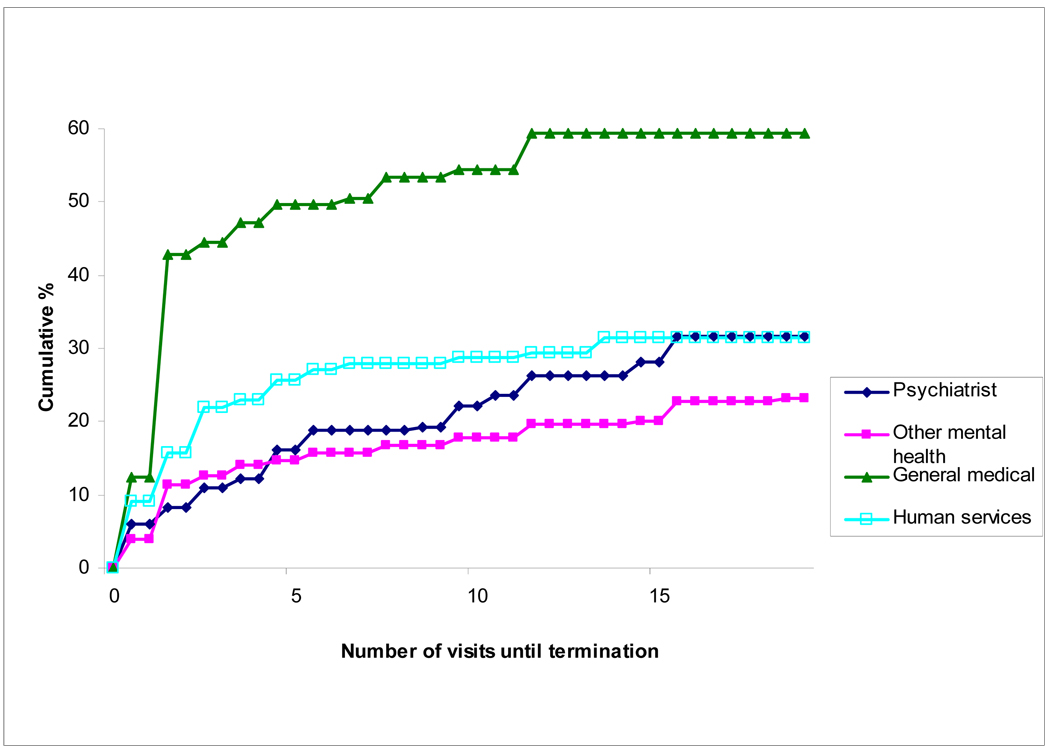
Results: Approximately one-fifth (22%) of patients quit treatment prematurely. The highest dropout rate was from treatment received in the general medical sector (32%), and the lowest was from treatment received by psychiatrists (15%). Dropout rates were intermediate from treatment in the human services sector (20%) and among patients seen by nonpsychiatrist mental health professionals (19%). Over 70% of all dropout occurred after the first or second visits. Mental health insurance was associated with low odds of dropout (odds ratio=.6, 95% confidence interval=.4-.9). Psychiatric comorbidity was associated with a trend toward dropout. Several patient characteristics differentially predicted dropout across treatment sectors and in early and later phases of treatment.
Conclusions: Roughly one-fifth of adults in mental health treatment dropped out before completing the recommended course of treatment. Dropout was most common in the general medical sector and varied by patient characteristics across treatment sectors. Interventions focused on high-risk patients and sectors that have higher dropout rates will likely be required to reduce the large proportion of patients who prematurely terminate treatment.
Figures
References
-
- Wang J. Mental health treatment dropout and its correlates in a general population sample. Medical Care. 2007;45:224–229. - PubMed
-
- Wang PS, Gilman SE, Guardino M, et al. Initiation of and adherence to treatment for mental disorders: examination of patient advocate group members in 11 countries. Medical Care. 2000;38:926–936. - PubMed
-
- Goldenberg V. Ranking the correlates of psychotherapy duration. Administration and Policy in Mental Health. 2002;29:201–214. - PubMed
-
- Hatchett GT, Han K, Cooker PG. Predicting premature termination from counseling using the Butcher Treatment Planning Inventory. Assessment. 2002;9:156–163. - PubMed
-
- Ogrodniczuk JS, Joyce AS, Piper WE. Strategies for reducing patient-initiated premature termination of psychotherapy. Harvard Review of Psychiatry. 2005;13:57–70. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DA016558/DA/NIDA NIH HHS/United States
- U01-MH60220/MH/NIMH NIH HHS/United States
- R01-MH070884/MH/NIMH NIH HHS/United States
- R03 TW006481/TW/FIC NIH HHS/United States
- R01 MH069864/MH/NIMH NIH HHS/United States
- R01-DA016558/DA/NIDA NIH HHS/United States
- R01-MH069864/MH/NIMH NIH HHS/United States
- DA 044780/DA/NIDA NIH HHS/United States
- U01 MH060220/MH/NIMH NIH HHS/United States
- R13-MH066849/MH/NIMH NIH HHS/United States
- R01 MH070884/MH/NIMH NIH HHS/United States
- U13 MH066849/MH/NIMH NIH HHS/United States
- R13 MH066849/MH/NIMH NIH HHS/United States
- K05 DA015799/DA/NIDA NIH HHS/United States
- R03-TW006481/TW/FIC NIH HHS/United States
