

Effect of a high-flow open nasal cannula system on obstructive sleep apnea in children
- PMID: 19564298
- PMCID: PMC2885875
- DOI: 10.1542/peds.2008-2824
Effect of a high-flow open nasal cannula system on obstructive sleep apnea in children
Abstract
Objective: Obstructive sleep apnea syndrome in children is associated with significant morbidity. Continuous positive airway pressure (CPAP) treats obstructive apnea in children, but is impeded by low adherence. We, therefore, sought to assess the effect of warm humidified air delivered through an open nasal cannula (treatment with nasal insufflation [TNI]) on obstructive sleep apnea in children with and without adenotonsillectomy.
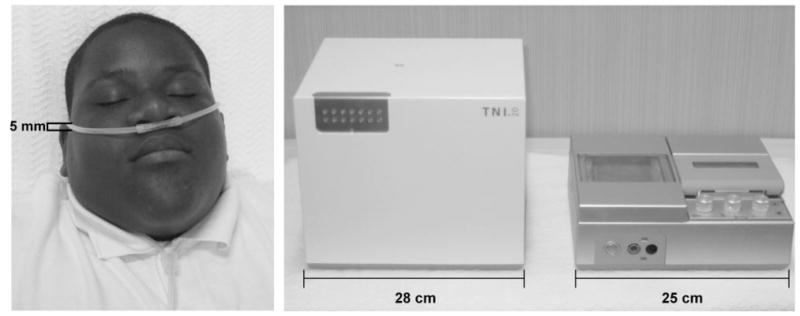
Methods: Twelve participants (age: 10 +/- 1 years; BMI: 35 +/- 14 kg/m(2)), with obstructive apnea-hypopnea syndrome ranging from mild to severe (2-36 events per hour) were administered 20 L/min of air through a nasal cannula. Standard sleep architecture, sleep-disordered breathing, and arousal indexes were assessed at baseline, on TNI, and on CPAP. Additional measures of the percentage of time with inspiratory flow limitation, respiratory rate, and inspiratory duty cycle were assessed at baseline and on TNI.
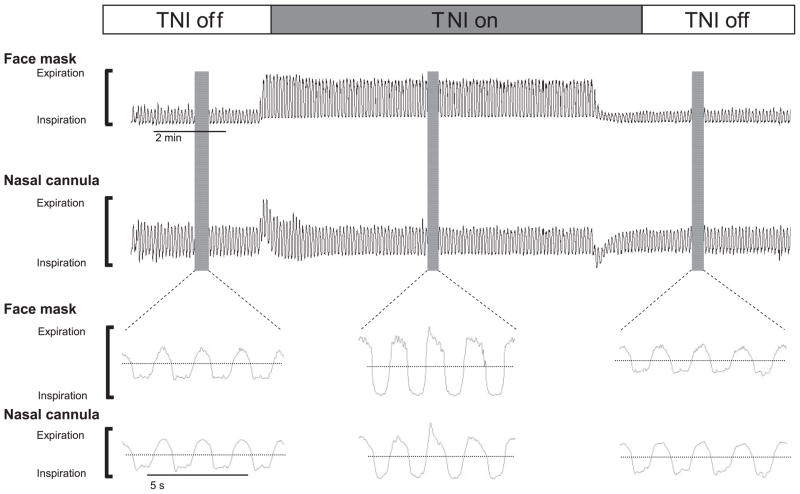
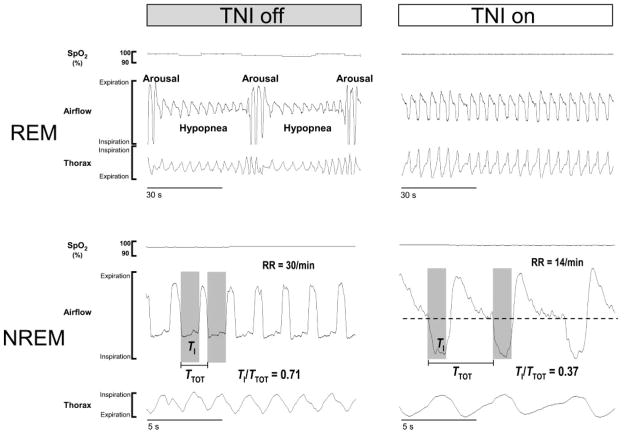
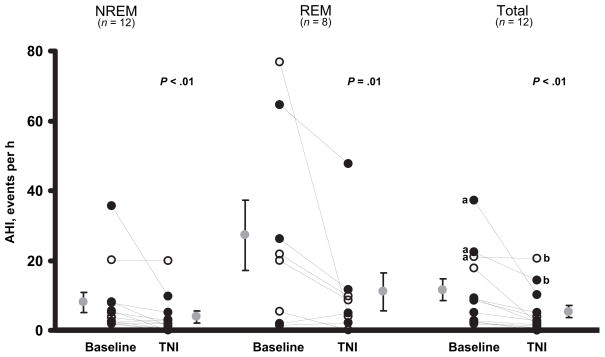
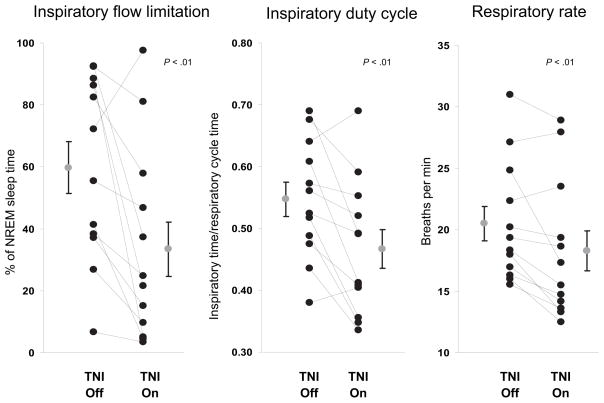
Results: TNI reduced the amount of inspiratory flow limitation, which led to a decrease in respiratory rate and inspiratory duty cycle. TNI improved oxygen stores and decreased arousals, which decreased the occurrence of obstructive apnea from 11 +/- 3 to 5 +/- 2 events per hour (P < .01). In the majority of children, the reduction in the apnea-hypopnea index on TNI was comparable to that on CPAP.
Conclusions: TNI offers an alternative to therapy to CPAP in children with mild-to-severe sleep apnea. Additional studies will be needed to determine the efficacy of this novel form of therapy.
Figures
References
-
- Eastwood PR, Szollosi I, Platt PR, Hillman DR. Comparison of upper airway collapse during general anesthesia and sleep. Lancet. 2002;359(9313):1207–1209. - PubMed
-
- Schwartz AR, Smith PL, Wise RA, Gold AR, Permutt S. Induction of upper airway occlusion in sleeping individuals with subatmospheric nasal pressure. J Appl Physiol. 1988;64(4):535–542. - PubMed
-
- Smith PL, Wise RA, Gold AR, Schwartz AR, Permutt S. Upper airway pressure-flow relationships in obstructive sleep apnea. J Appl Physiol. 1988;64(2):789–795. - PubMed
-
- Chervin RD, Archbold KH. Hyperactivity and polysomnographic findings in children evaluated for sleep-disordered breathing. Sleep. 2001;24(3):313–320. - PubMed
-
- Owens J, Opipari L, Nobile C, Spirito A. Sleep and daytime behavior in children with obstructive sleep apnea and behavioral sleep disorders. Pediatrics. 1998;102(5):1178–1184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
