

Prevention of pulmonary hypertension by Angiotensin-converting enzyme 2 gene transfer
- PMID: 19564552
- PMCID: PMC2732127
- DOI: 10.1161/HYPERTENSIONAHA.108.125468
Prevention of pulmonary hypertension by Angiotensin-converting enzyme 2 gene transfer
Abstract
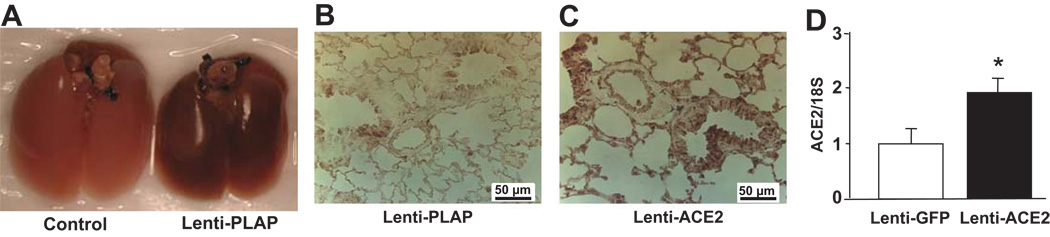
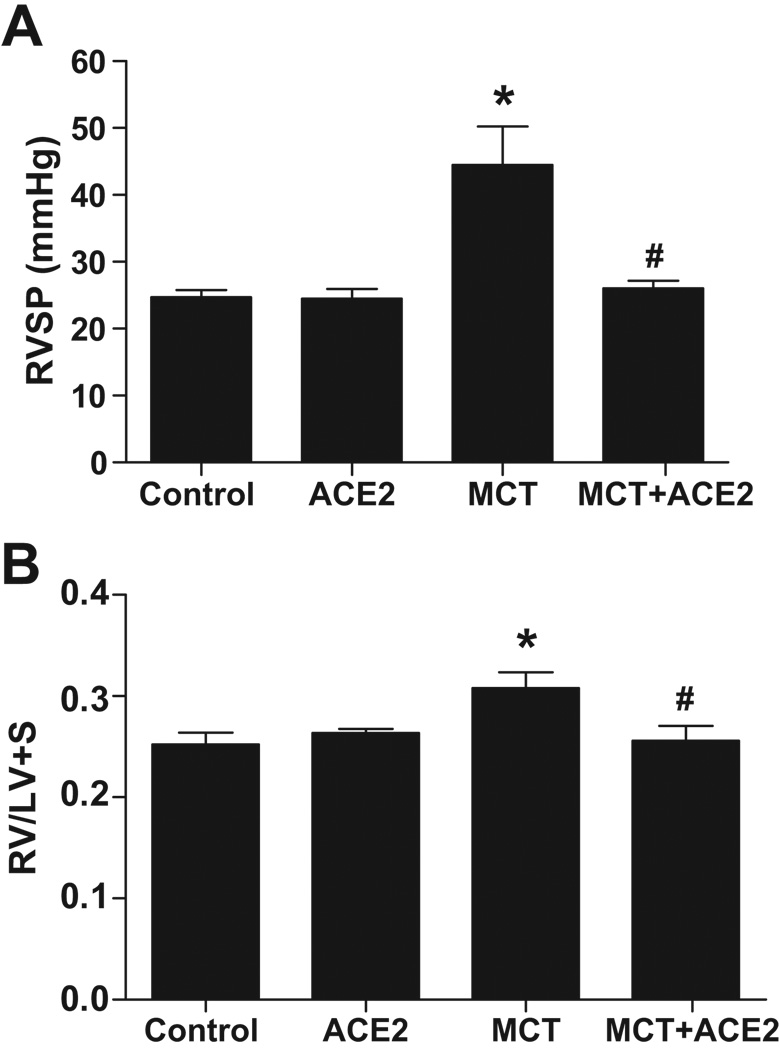
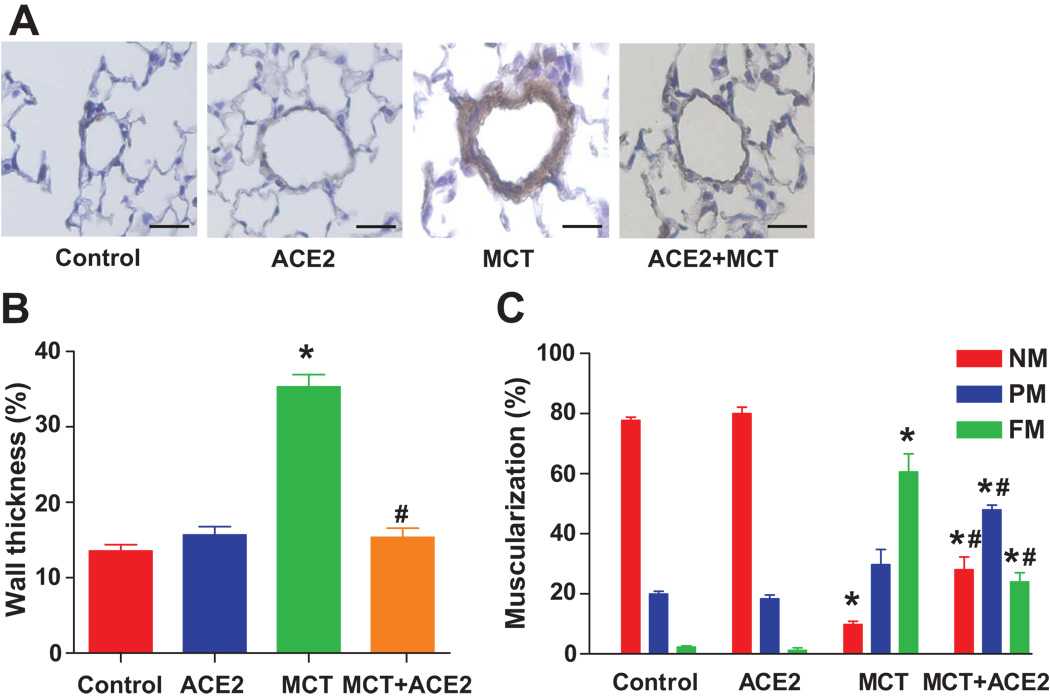
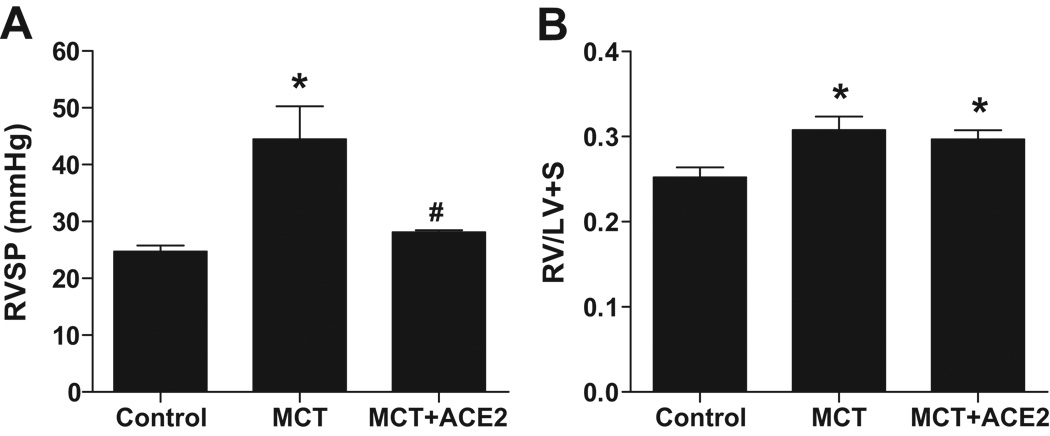
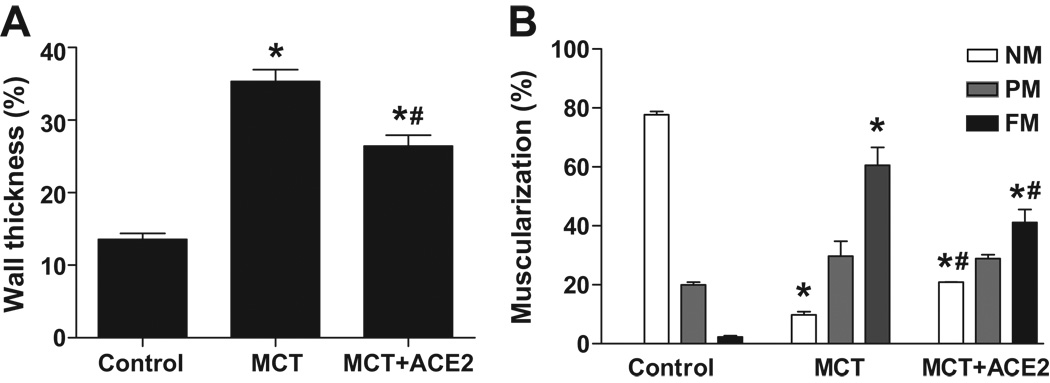
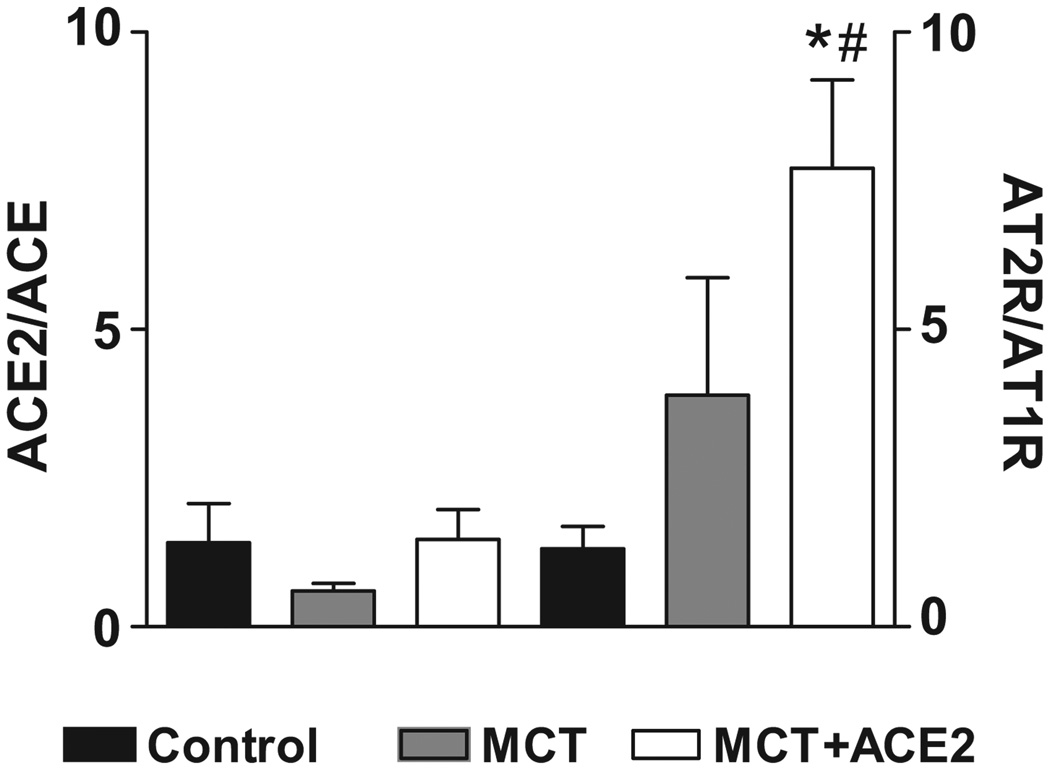
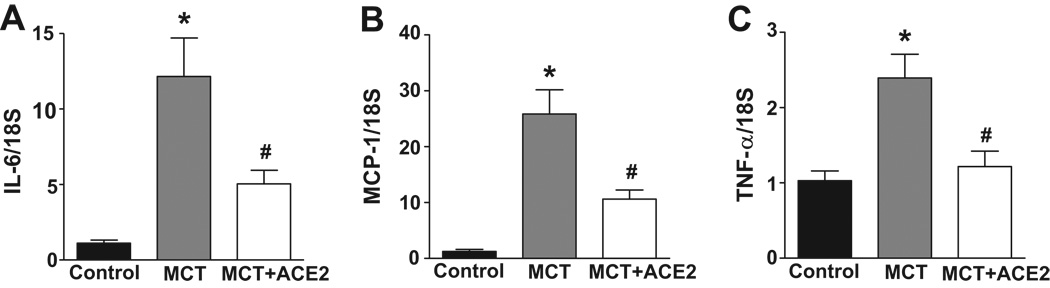
In spite of recent advancements in the treatment of pulmonary hypertension, successful control has yet to be accomplished. The abundant presence of angiotensin-converting enzyme 2 (ACE2) in the lungs and its impressive effect in the prevention of acute lung injury led us to test the hypothesis that pulmonary overexpression of this enzyme could produce beneficial outcomes against pulmonary hypertension. Monocrotaline (MCT) treatment of mice for 8 weeks resulted in significant increases in right ventricular systolic pressure, right ventricle:left ventricle plus septal weight ratio, and muscularization of pulmonary vessels. Administration of a lentiviral vector containing ACE2, 7 days before MCT treatment prevented the increases in right ventricular systolic pressure (control: 25+/-1 mm Hg; MCT: 44+/-5 mm Hg; MCT+ACE2: 26+/-1 mm Hg; n=6; P<0.05) and right ventricle:left ventricle plus septal weight ratio (control: 0.25+/-0.01; MCT: 0.31+/-0.01; MCT+ACE2: 0.26+/-0.01; n=8; P<0.05). A significant attenuation in muscularization of pulmonary vessels induced by MCT was also observed in animals overexpressing ACE2. These beneficial effects were associated with an increase in the angiotensin II type 2 receptor:angiotensin II type 1 receptor mRNA ratio. Also, pulmonary hypertension-induced increases in proinflammatory cytokines were significantly attenuated by lentiviral vector-containing ACE2 treatment. Furthermore, ACE2 gene transfer in mice after 6 weeks of MCT treatment resulted in a significant reversal of right ventricular systolic pressure. These observations demonstrate that ACE2 overexpression prevents and reverses right ventricular systolic pressure and associated pathophysiology in MCT-induced pulmonary hypertension by a mechanism involving a shift from the vasoconstrictive, proliferative, and fibrotic axes to the vasoprotective axis of the renin-angiotensin system and inhibition of proinflammatory cytokines.
Figures
References
-
- Coggins MP, Bloch KD. Nitric oxide in the pulmonary vasculature. Arterioscler Thromb Vasc Biol. 2007;27:1877–1885. - PubMed
-
- Stenmark KR, Fagan KA, Frid MG. Hypoxia-induced pulmonary vascular remodeling: cellular and molecular mechanisms. Circ Res. 2006;99:675–691. - PubMed
-
- Marshall RP. The pulmonary renin-angiotensin system. Curr Pharm Des. 2003;9:715–722. - PubMed
-
- Dezsö B, Nielsen AH, Poulsen K. Identification of renin in resident alveolar macrophages and monocytes: HPLC and immunohistochemical study. J Cell Sci. 1988;91:155–159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
