

Contemporary management of atrial fibrillation: update on anticoagulation and invasive management strategies
- PMID: 19567719
- PMCID: PMC2704137
- DOI: 10.1016/S0025-6196(11)60754-4
Contemporary management of atrial fibrillation: update on anticoagulation and invasive management strategies
Abstract
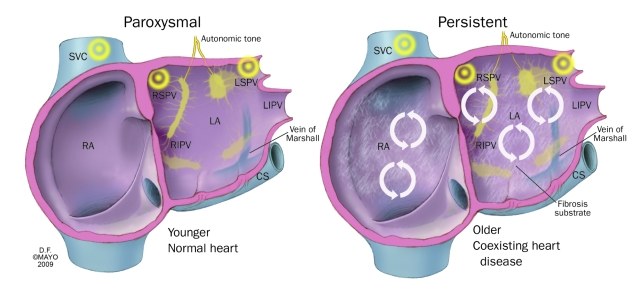
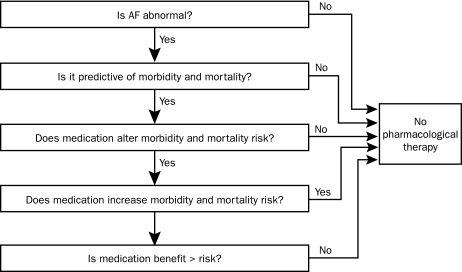
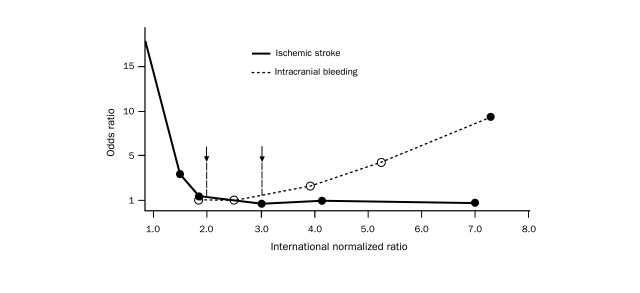
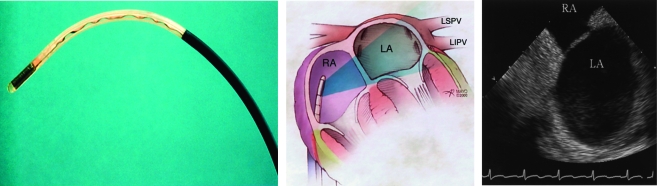
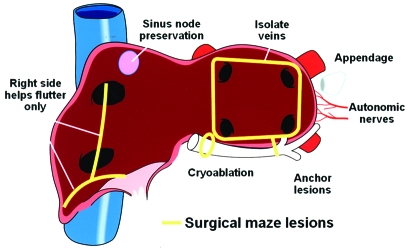
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinical practice. Its increasing prevalence, particularly among the elderly, renders it one of the most serious current medical epidemics. Several management questions confront the clinician treating a patient with AF: Should the condition be treated? Is the patient at risk of death or serious morbidity as a result of this diagnosis? If treatment is necessary, is rate control or rhythm control superior? Which patients need anticoagulation therapy, and for how long? This review of articles obtained by a search of the PubMed and MEDLINE databases presents the available evidence that can guide the clinician in answering these questions. After discussing the merits of available therapy, including medications aimed at controlling rate, rhythm, or both, we focus on the present status of ablative therapy for AF. Catheter ablation, particularly targeting the pulmonary veins, is being increasingly performed, although the precise indications for this approach and its effectiveness and safety are being actively investigated. We briefly discuss other invasive options that are less frequently used, such as pacemakers, defibrillators, left atrial appendage closure devices, and the surgical maze procedure.
Figures

References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285(18):2370-2375 - PubMed
-
- Jahangir A, Lee V, Friedman PA, et al. Long-term progression and outcomes with aging in patients with lone atrial fibrillation: a 30-year follow-up study. Circulation 2007;115(24):3050-3056 Epub 2007 Jun 4. - PubMed
-
- European Heart Rhythm Association. Heart Rhythm Society. Fuster V, Rydén LE, Cannom DS, et al. American College of Cardiology. American Heart Association Task Force on Practice Guidelines. European Society of Cardiology Committee for Practice Guidelines. Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation) [published correction appears in J Am Coll Cardiol. 2007;50(6):562] J Am Coll Cardiol. 2006;48(4):854-906 - PubMed
-
- Al-Khatib SM, Wilkinson WE, Sanders LL, McCarthy EA, Pritchett EL. Observations on the transition from intermittent to permanent atrial fibrillation. Am Heart J. 2000;140(1):142-145 - PubMed
-
- Kerr CR, Humphries KH, Talajic M, et al. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2005;149(3):489-496 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
