

Phase Ib study of NGR-hTNF, a selective vascular targeting agent, administered at low doses in combination with doxorubicin to patients with advanced solid tumours
- PMID: 19568235
- PMCID: PMC2720203
- DOI: 10.1038/sj.bjc.6605162
Phase Ib study of NGR-hTNF, a selective vascular targeting agent, administered at low doses in combination with doxorubicin to patients with advanced solid tumours
Abstract
Background: Asparagine-glycine-arginine-human tumour necrosis factor (NGR-hTNF) is a vascular targeting agent exploiting a tumour-homing peptide (NGR) that selectively binds to aminopeptidase N/CD13, overexpressed on tumour blood vessels. Significant preclinical synergy was shown between low doses of NGR-TNF and doxorubicin.
Methods: The primary aim of this phase I trial was to verify the safety of low-dose NGR-hTNF combined with doxorubicin in treating refractory/resistant solid tumours. Secondary objectives included pharmacokinetics (PKs), pharmacodynamics, and clinical activity. In all 15 patients received NGR-hTNF (0.2-0.4-0.8-1.6 microg m(-2)) and doxorubicin (60-75 mg m(-2)), both given intravenously every 3 weeks.
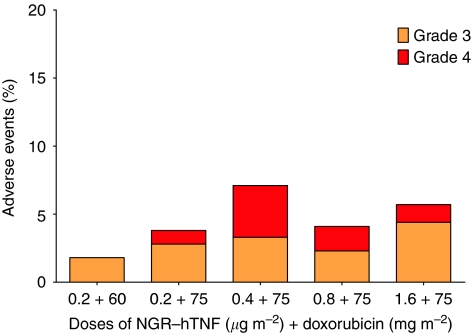
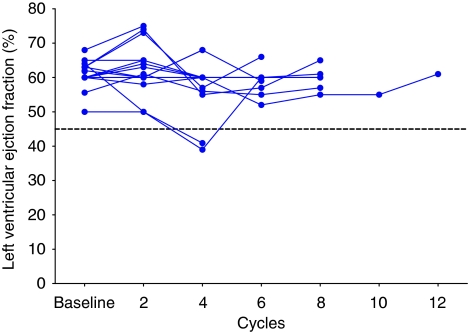
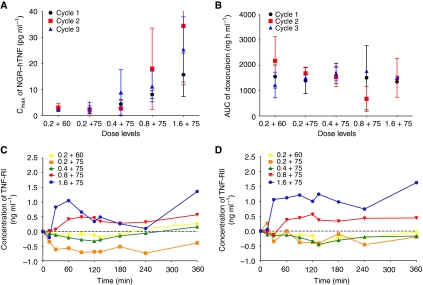
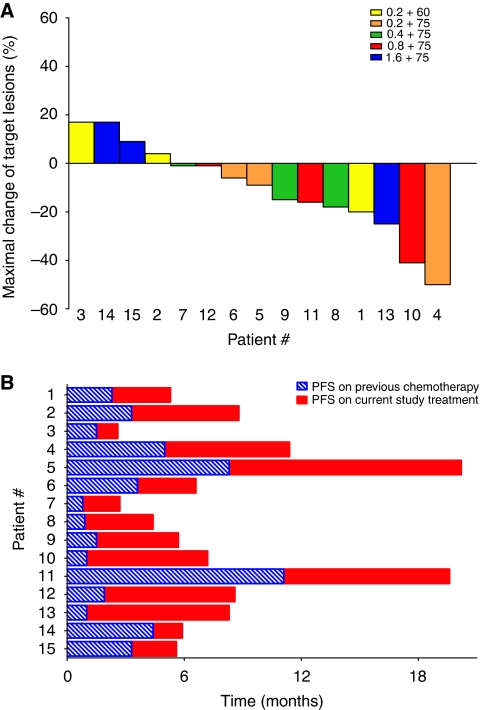
Results: No dose-limiting toxicity occurred and the combination was well tolerated. Around two cases of neutropenic fevers, lasting 2 days, and two cases of cardiac ejection-fraction drops, one asymptomatic and the other symptomatic, were registered. Only 11% of the adverse events were related to NGR-hTNF and were short-lasting and mild-to-moderate in severity. There was no apparent PK interaction and the shedding of soluble TNF-receptors did not increase to 0.8 microg m(-2). One partial response (7%), at dose level 0.8 microg m(-2), and 10 stable diseases (66%), lasting for a median duration of 5.6 months, were observed.
Conclusions: NGR-hTNF plus doxorubicin was administered safely and showed promising activity in patients pre-treated with anthracyclines. The dose level of 0.8 microg m(-2) NGR-hTNF plus doxorubicin 75 mg m(-2) was selected for phase II development.
Figures
References
-
- Carver JR, Shapiro CL, Ng A, Jacobs L, Schwartz C, Virgo KS, Hagerty KL, Somerfield MR, Vaughn DJ, for the ASCO Cancer Survivorship Expert Panel (2007) American Society of Clinical Oncology clinical evidence review on the ongoing care of adult cancer survivors: cardiac and pulmonary late effects. J Clin Oncol 25: 3991–4008 - PubMed
-
- Corti A, Ponzoni M (2004) Tumor vascular targeting with tumor necrosis factor alpha and chemotherapeutic drugs. Ann N Y Acad Sci 1028: 104–112 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
