

Gemcitabine-based chemogene therapy for pancreatic cancer using Ad-dCK::UMK GDEPT and TS/RR siRNA strategies
- PMID: 19568409
- PMCID: PMC2697350
- DOI: 10.1593/neo.81686
Gemcitabine-based chemogene therapy for pancreatic cancer using Ad-dCK::UMK GDEPT and TS/RR siRNA strategies
Abstract
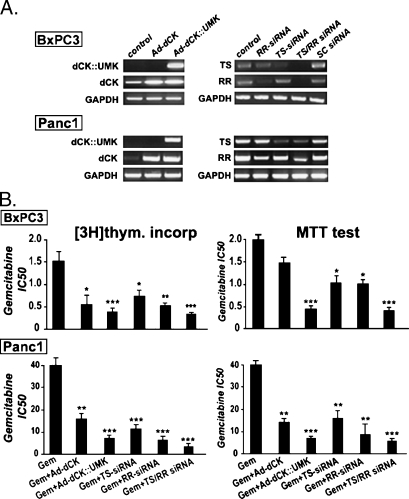
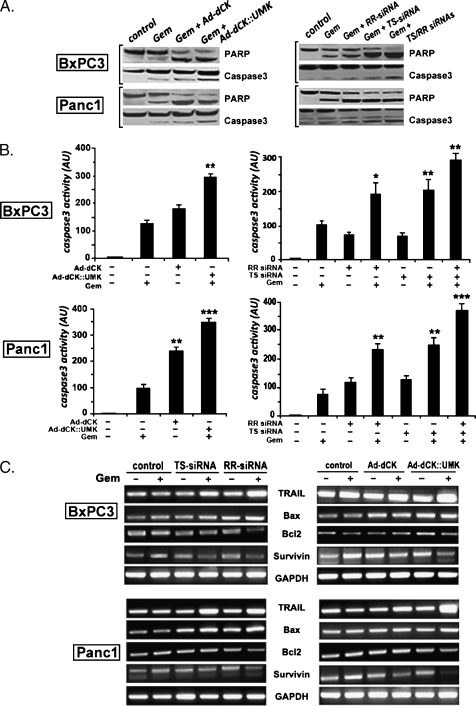
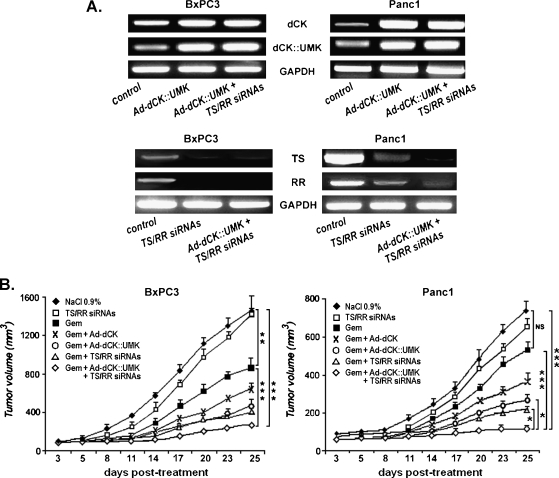
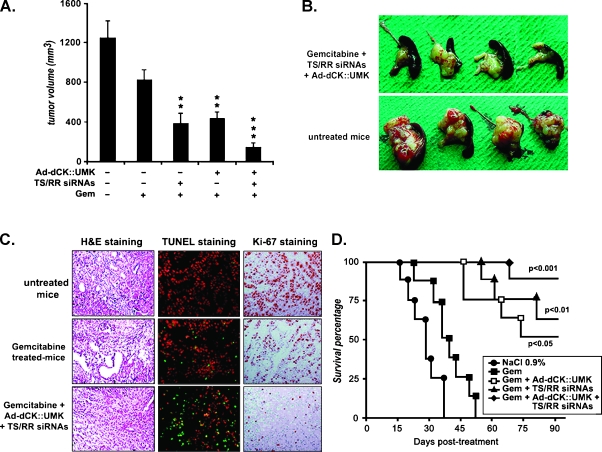
Gemcitabine is a first-line agent for advanced pancreatic cancer therapy. However, its efficacy is often limited by its poor intracellular metabolism and chemoresistance. To exert its antitumor activity, gemcitabine requires to be converted to its active triphosphate form. Thus, our aim was to improve gemcitabine activation using gene-directed enzyme prodrug therapy based on gemcitabine association with the deoxycytidine kinase::uridine monophosphate kinase fusion gene (dCK::UMK) and small interference RNA directed against ribonucleotide reductase (RRM2) and thymidylate synthase (TS). In vitro, cytotoxicity was assessed by 3-[4,5-dimethylthiazol-2-yl]-3,5-diphenyl tetrazolium bromide and [(3)H]thymidine assays. Apoptosis-related gene expression and activity were analyzed by reverse transcription-polymerase chain reaction, Western blot, and ELISA. For in vivo studies, the treatment efficacy was evaluated on subcutaneous and orthotopic pancreatic tumor models. Our data indicated that cell exposure to gemcitabine induced a down-regulation of dCK expression and up-regulation of TS and RR expression in Panc1-resistant cells when compared with BxPc3- and HA-hpc2-sensitive cells. The combination of TS/RRM2 small interference RNA with Ad-dCK::UMK induced a 40-fold decrease of gemcitabine IC(50) in Panc1 cells. This strong sensitization was associated to apoptosis induction with a remarkable increase in TRAIL expression and a diminution of gemcitabine-induced nuclear factor-kappaB activity. In vivo, the gemcitabine-based tritherapy strongly reduced tumor volumes and significantly prolonged mice survival. Moreover, we observed an obvious increase of apoptosis and decrease of cell proliferation in tumors receiving the tritherapy regimens. Together, these findings suggest that simultaneous TS/RRM2-gene silencing and dCK::UMK gene overexpression markedly improved gemcitabine's therapeutic activity. Clearly, this combined strategy warrants further investigation.
Figures



References
-
- Yeo TP, Hruban RH, Leach SD, Wilentz RE, Sohn TA, Kern SE, Iacobuzio-Donahue CA, Maitra A, Goggins M, Canto MI, et al. Pancreatic cancer. Curr Probl Cancer. 2002;26:176–275. - PubMed
-
- Kollmannsberger C, Peters HD, Fink U. Chemotherapy in advanced pancreatic adenocarcinoma. Cancer Treat Rev. 1998;24:133–156. - PubMed
-
- Burris HA, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, Cripps MC, Portenoy RK, Storniolo AM, Tarassoff P, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreatic cancer: a randomized-trial. J Clin Oncol. 1997;15:2403–2413. - PubMed
-
- Burris H, Storniolo AM. Assessing clinical benefit in the treatment of pancreas cancer: gemcitabine compared to 5-fluorouracil. Eur J Cancer. 1997;33(Suppl):18–22. - PubMed
-
- Rothenberg ML, Moore MJ, Cripps MC, Andersen JS, Portenoy RK, Burris HA, III, Green MR, Tarassoff PG, Brown TD, Casper ES, et al. A phase II trial of gemcitabine in patients with 5-FU-refractory pancreas cancer. Ann Oncol. 1996;7:347–353. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous