

Effects of clinical pathways in the joint replacement: a meta-analysis
- PMID: 19570193
- PMCID: PMC2715423
- DOI: 10.1186/1741-7015-7-32
Effects of clinical pathways in the joint replacement: a meta-analysis
Abstract
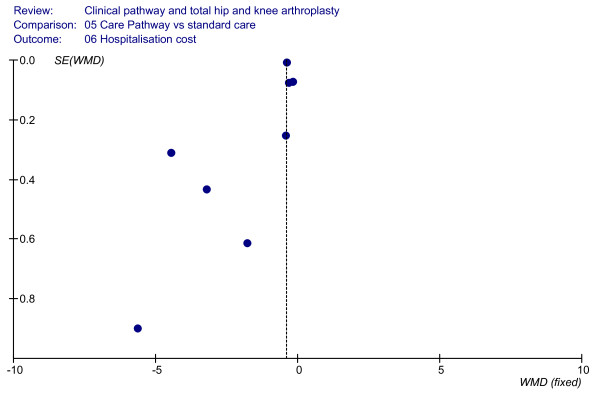
Background: A meta-analysis was performed to evaluate the use of clinical pathways for hip and knee joint replacements when compared with standard medical care. The impact of clinical pathways was evaluated assessing the major outcomes of in-hospital hip and knee joint replacement processes: postoperative complications, number of patients discharged at home, length of in-hospital stay and direct costs.
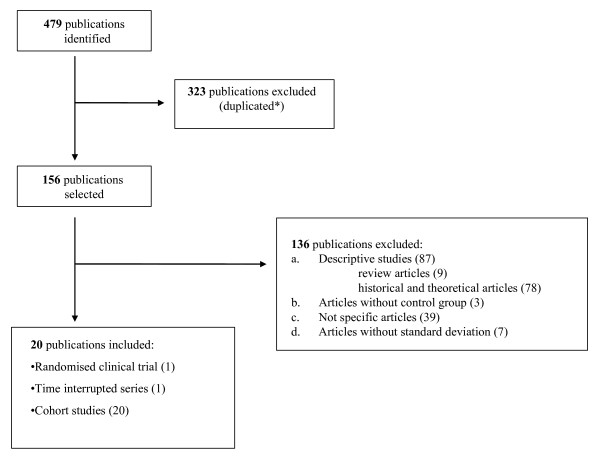
Methods: Medline, Cinahl, Embase and the Cochrane Central Register of Controlled Trials were searched. The search was performed from 1975 to 2007. Each study was assessed independently by two reviewers. The assessment of methodological quality of the included studies was based on the Jadad methodological approach and on the New Castle Ottawa Scale. Data analysis abided by the guidelines set out by The Cochrane Collaboration regarding statistical methods. Meta-analyses were performed using RevMan software, version 4.2.
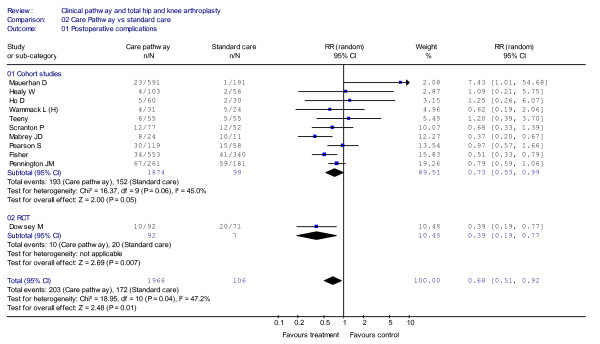
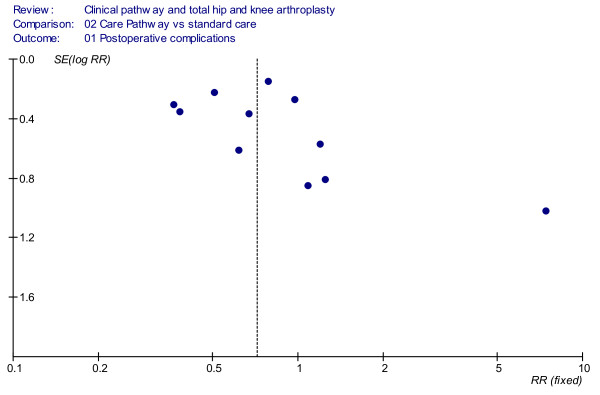
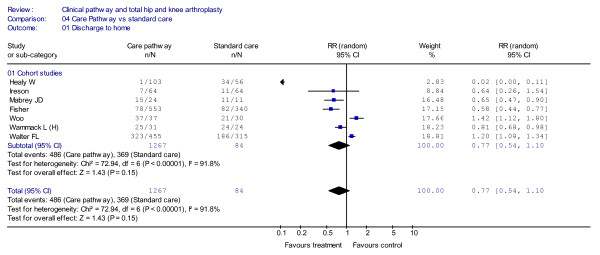
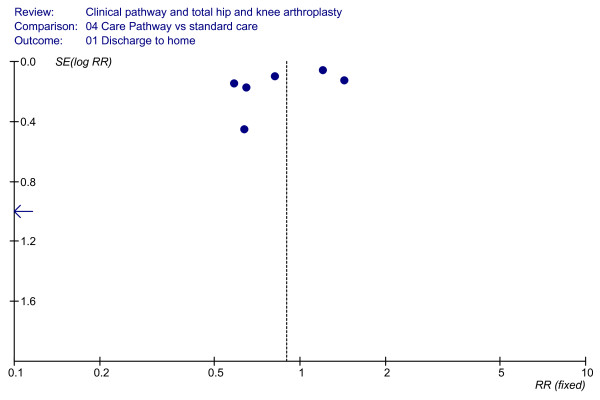
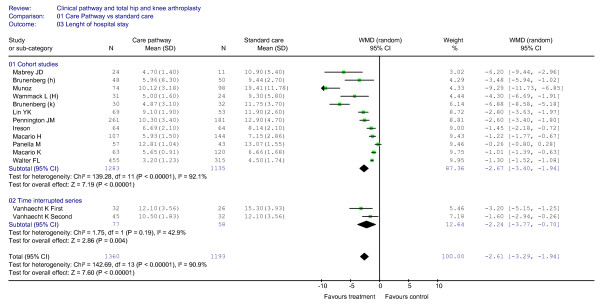
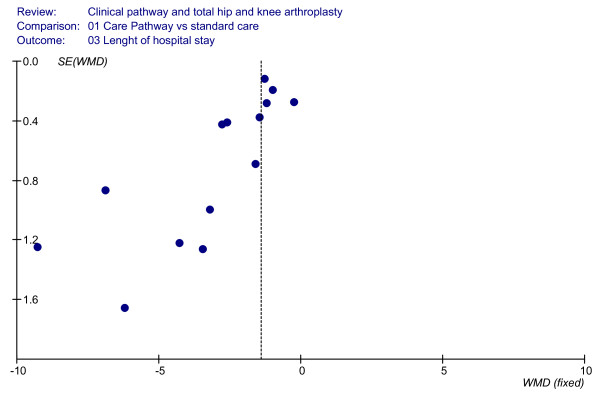
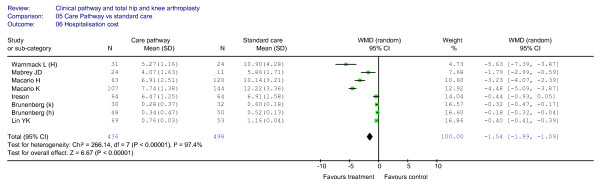
Results: Twenty-two studies met the study inclusion criteria and were included in the meta-analysis for a total sample of 6,316 patients. The aggregate overall results showed significantly fewer patients suffering postoperative complications in the clinical pathways group when compared with the standard care group. A shorter length of stay in the clinical pathway group was also observed and lower costs during hospital stay were associated with the use of the clinical pathways. No significant differences were found in the rates of discharge to home.
Conclusion: The results of this meta-analysis show that clinical pathways can significantly improve the quality of care even if it is not possible to conclude that the implementation of clinical pathways is a cost-effective process, because none of the included studies analysed the cost of the development and implementation of the pathways. Based on the results we assume that pathways have impact on the organisation of care if the care process is structured in a standardised way, teams critically analyse the actual organisation of the process and the multidisciplinary team is highly involved in the re-organisation. Further studies should focus on the evaluation of pathways as complex interventions to help to understand which mechanisms within the clinical pathways can really improve the quality of care. With the need for knee and hip joint replacement on the rise, the use of clinical pathways might contribute to better quality of care and cost-effectiveness.
Figures
References
-
- American Academy of Orthopaedic Surgeons (AAOS) Information about hip replacements. 2002. http://www.aaos.org/research/stats/Hip_Facts.pdf
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
