

Azathioprine for ocular inflammatory diseases
- PMID: 19570522
- PMCID: PMC2753718
- DOI: 10.1016/j.ajo.2009.05.008
Azathioprine for ocular inflammatory diseases
Abstract
Purpose: To evaluate treatment outcomes of azathioprine for noninfectious ocular inflammatory diseases.
Design: Retrospective cohort study.
Methods: Medical records of 145 patients starting azathioprine as a sole noncorticosteroid immunosuppressant at 4 tertiary uveitis services were reviewed. Main outcome measures included control of ocular inflammation, sustained control after tapering prednisone to </= 10 mg/day, and discontinuation of treatment because of side effects.
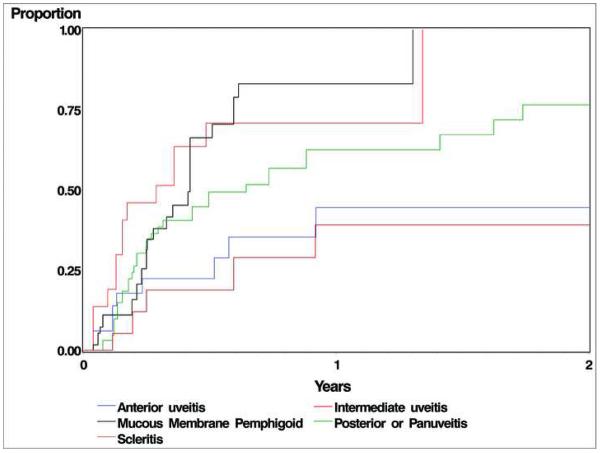
Results: Among 145 patients (255 eyes) treated with azathioprine, 63% had uveitis, 23% had mucous membrane pemphigoid, 11% had scleritis, and 3% had other inflammatory diseases. By Kaplan-Meier analysis, 62% (95% confidence interval [CI], 50% to 74%) of patients with active disease initially gained complete inactivity of inflammation sustained over at least 28 days within 1 year of therapy, and 47% (95% CI, 37% to 58%) tapered systemic corticosteroids to </= 10 mg daily while maintaining control of inflammation within 1 year of therapy. Treatment success was most common for intermediate uveitis (90% with sustained inactivity within 1 year; 95% CI, 64% to 99%). Over the median follow-up of 230 days (interquartile range, 62 to 679 days), azathioprine was discontinued at a rate of 0.45 per person-years (/PY): 0.16/PY because of side effects, 0.10/PY because of ineffectiveness, 0.09/PY because of disease remission, and 0.10/PY because of unspecified causes.
Conclusions: Azathioprine was moderately effective as a single corticosteroid-sparing immunosuppressive agent in terms of control of inflammation and corticosteroid-sparing benefits, but required several months to achieve treatment goals; it seems especially useful for patients with intermediate uveitis. Treatment-limiting side effects occurred in approximately one-fourth of patients within 1 year, but typically were reversible.
Figures
References
-
- Jabs DA, Rosenbaum JT, Foster CS, et al. Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations of an expert panel. Am J Ophthalmol. 2000;130:492–513. Medline. doi:10.1016/S0002-9394(00)00659-0. - PubMed
-
- Ward JR. Role of disease-modifying antirheumatic drugs versus cytotoxic agents in the therapy of rheumatoid arthritis. Am J Med. 1988;85:39–44. Medline. doi:10.1016/0002-9343(88)90361-0. - PubMed
-
- Danovitch GM. Choice of immunosuppressive drugs and individualization of immunosuppressive therapy for kidney transplant patients. Transplant Proc. 1999;31:2S–6S. Medline. doi:10.1016/S0041-1345(99)00840-4. - PubMed
-
- Wise M, Callen JP. Azathioprine: a guide for the management of dermatology patients. Dermatol Ther. 2007;20:206–215. Medline. doi:10.1111/j.1529-8019.2007.00134.x. - PubMed
-
- Gisbert JP, Nino P, Cara C, Rodrigo L. Comparative effectiveness of azathioprine in Crohn's disease and ulcerative colitis: prospective, long-term, follow-up study of 394 patients. Aliment Pharmacol Ther. 2008;28:228–238. Medline. doi:10.1111/j.1365-2036.2008.03732.x. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
