

Utility of a commercially available multiplex real-time PCR assay to detect bacterial and fungal pathogens in febrile neutropenia
- PMID: 19571034
- PMCID: PMC2725651
- DOI: 10.1128/JCM.00491-09
Utility of a commercially available multiplex real-time PCR assay to detect bacterial and fungal pathogens in febrile neutropenia
Abstract
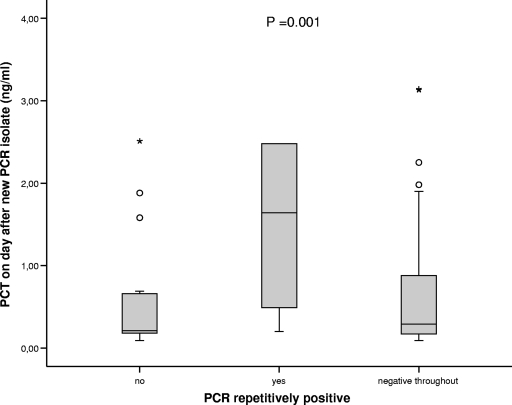
Infection is the main treatment-related cause of mortality in cancer patients. Rapid and accurate diagnosis to facilitate specific therapy of febrile neutropenia is therefore urgently warranted. Here, we evaluated a commercial PCR-based kit to detect the DNA of 20 different pathogens (SeptiFast) in the setting of febrile neutropenia after chemotherapy. Seven hundred eighty-four serum samples of 119 febrile neutropenic episodes (FNEs) in 70 patients with hematological malignancies were analyzed and compared with clinical, microbiological, and biochemical findings. In the antibiotic-naïve setting, bacteremia was diagnosed in 34 FNEs and 11 of them yielded the same result in the PCR. Seventy-three FNEs were negative in both systems, leading to an overall agreement in 84 of 119 FNEs (71%). During antibiotic therapy, positivity in blood culture occurred only in 3% of cases, but the PCR yielded a positive result in 15% of cases. In six cases the PCR during antibiotic treatment detected a new pathogen repetitively; this was accompanied by a significant rise in procalcitonin levels, suggestive of a true detection of infection. All patients with probable invasive fungal infection (IFI; n = 3) according to the standards of the European Organization for Research and Treatment of Cancer had a positive PCR result for Aspergillus fumigatus; in contrast there was only one positive result for Aspergillus fumigatus in an episode without signs and symptoms of IFI. Our results demonstrate that the SeptiFast kit cannot replace blood cultures in the diagnostic workup of FNEs. However, it might be helpful in situations where blood cultures remain negative (e.g., during antimicrobial therapy or in IFI).
Figures

Similar articles
-
Multiplex blood PCR in combination with blood cultures for improvement of microbiological documentation of infection in febrile neutropenia.J Clin Microbiol. 2010 Oct;48(10):3510-6. doi: 10.1128/JCM.00147-10. Epub 2010 Aug 18. J Clin Microbiol. 2010. PMID: 20720024 Free PMC article.
-
Diagnostic value of PCR analysis of bacteria and fungi from blood in empiric-therapy-resistant febrile neutropenia.J Clin Microbiol. 2010 Jun;48(6):2030-6. doi: 10.1128/JCM.01700-09. Epub 2010 Apr 14. J Clin Microbiol. 2010. PMID: 20392911 Free PMC article.
-
Evaluation of pan-fungal PCR assay and Aspergillus antigen detection in the diagnosis of invasive fungal infections in high risk paediatric cancer patients.Med Mycol. 2006 Dec;44(8):733-9. doi: 10.1080/13693780600939955. Med Mycol. 2006. PMID: 17127630
-
New molecular and surrogate biomarker-based tests in the diagnosis of bacterial and fungal infection in febrile neutropenic patients.Curr Opin Infect Dis. 2010 Dec;23(6):567-77. doi: 10.1097/QCO.0b013e32833ef7d1. Curr Opin Infect Dis. 2010. PMID: 20827189 Review.
-
The current spectrum of infection in cancer patients with chemotherapy related neutropenia.Infection. 2014 Feb;42(1):5-13. doi: 10.1007/s15010-013-0525-9. Epub 2013 Aug 23. Infection. 2014. PMID: 23975584 Review.
Cited by
-
Multiplex PCR for rapid and improved diagnosis of bloodstream infections in liver transplant recipients.J Clin Microbiol. 2012 Jun;50(6):2069-71. doi: 10.1128/JCM.00745-12. Epub 2012 Apr 4. J Clin Microbiol. 2012. PMID: 22493334 Free PMC article.
-
Multiplex PCR to diagnose bloodstream infections in patients admitted from the emergency department with sepsis.J Clin Microbiol. 2010 Jan;48(1):26-33. doi: 10.1128/JCM.01447-09. Epub 2009 Oct 21. J Clin Microbiol. 2010. PMID: 19846634 Free PMC article.
-
Performance of the LightCycler SeptiFast test Mgrade in detecting microbial pathogens in purulent fluids.J Clin Microbiol. 2011 Aug;49(8):2988-91. doi: 10.1128/JCM.00359-11. Epub 2011 Jun 29. J Clin Microbiol. 2011. PMID: 21715593 Free PMC article.
-
SeptiFast versus blood culture in clinical routine - A report on 3 years experience.Wien Klin Wochenschr. 2017 Jun;129(11-12):427-434. doi: 10.1007/s00508-017-1181-3. Epub 2017 Feb 27. Wien Klin Wochenschr. 2017. PMID: 28243751 Free PMC article.
-
Evaluation of the Magicplex™ Sepsis Real-Time Test for the Rapid Diagnosis of Bloodstream Infections in Adults.Front Cell Infect Microbiol. 2019 Mar 12;9:56. doi: 10.3389/fcimb.2019.00056. eCollection 2019. Front Cell Infect Microbiol. 2019. PMID: 30931259 Free PMC article.
References
-
- Ammann, R. A., F. Zucol, C. Aebi, F. K. Niggli, T. Kuhne, and D. Nadal. 2007. Real-time broad-range PCR versus blood culture. A prospective pilot study in pediatric cancer patients with fever and neutropenia. Support Care Cancer 15637-641. - PubMed
-
- Ascioglu, S., J. H. Rex, B. de Pauw, J. E. Bennett, J. Bille, F. Crokaert, D. W. Denning, J. P. Donnelly, J. E. Edwards, Z. Erjavec, D. Fiere, O. Lortholary, J. Maertens, J. F. Meis, T. F. Patterson, J. Ritter, D. Selleslag, P. M. Shah, D. A. Stevens, and T. J. Walsh. 2002. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin. Infect. Dis. 347-14. - PubMed
-
- Fleischhack, G., I. Kambeck, D. Cipic, C. Hasan, and U. Bode. 2000. Procalcitonin in paediatric cancer patients: its diagnostic relevance is superior to that of C-reactive protein, interleukin 6, interleukin 8, soluble interleukin 2 receptor and soluble tumour necrosis factor receptor II. Br. J. Haematol. 1111093-1102. - PubMed
-
- Grace, C. J., J. Lieberman, K. Pierce, and B. Littenberg. 2001. Usefulness of blood culture for hospitalized patients who are receiving antibiotic therapy. Clin. Infect. Dis. 321651-1655. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
