

Outcomes after arthroscopic repair of type-II SLAP lesions
- PMID: 19571081
- PMCID: PMC2702251
- DOI: 10.2106/JBJS.H.00205
Outcomes after arthroscopic repair of type-II SLAP lesions
Abstract
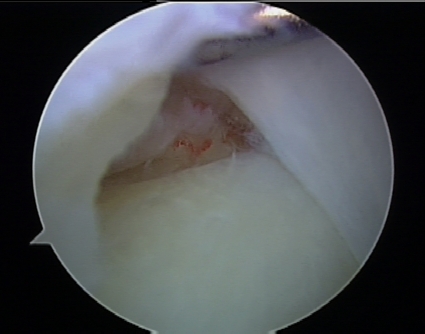
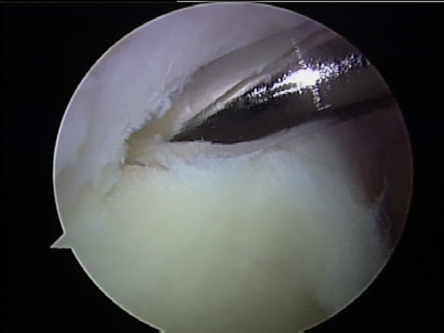
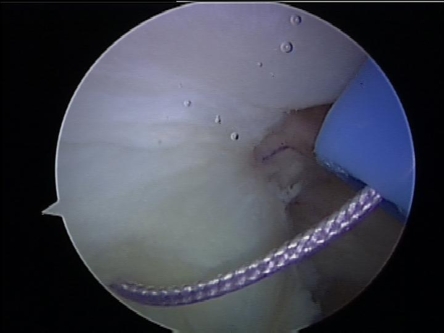
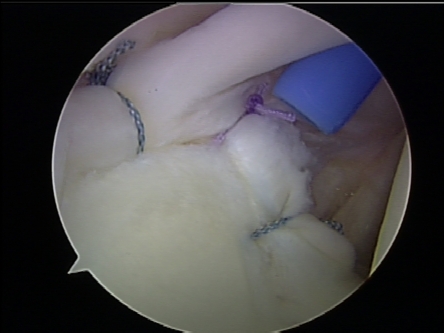
Background: To our knowledge, there has been no prospective study on the results of arthroscopic repair of superior labrum-biceps anchor complex (SLAP) tears with use of modern techniques. The purpose of the present study was to prospectively evaluate the minimum two-year results for patients with type-II SLAP tears that were treated with arthroscopic suture anchor fixation.
Methods: Forty-seven patients with symptomatic type-II SLAP tears were evaluated preoperatively and at least two years postoperatively with use of the American Shoulder and Elbow Surgeons (ASES) and L'Insalata outcomes instruments and physical examination. The study group included thirty-nine male and eight female patients with a mean age of thirty-six years; thirty-four of the forty-seven patients were athletes. Patients with rotator cuff tears requiring repair or concomitant shoulder instability were excluded.
Results: At an average of 2.7 years, the median ASES and L'Insalata scores were 97 and 93, respectively, compared with baseline scores of 62 and 65 (p < 0.05). The median patient-reported satisfaction rating was 9 (of 10); forty-one patients (87%) rated the outcome as good or excellent. The median patient-reported satisfaction rating was significantly higher for patients with a discrete traumatic etiology than for those with an atraumatic etiology (9 compared with 7); however, there was no significant difference between these groups in terms of the ASES or L'Insalata outcome scores. Overall, twenty-five (74%) of the thirty-four athletes were able to return to their preinjury level of competition, whereas eleven (92%) of the twelve athletes who reported a discrete traumatic event were able to return to their previous level of competition. There were five complications, including four cases of refractory postoperative stiffness.
Conclusions: Our findings indicate that favorable outcomes can be anticipated in the majority of patients after arthroscopic SLAP lesion repair. While only three of four patients overall may be capable of returning fully to their previous level of competition, patients with a distinct traumatic etiology have a greater likelihood of a successful return to sports.
Figures
References
-
- Andrews JR, Carson WG Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13:337-41. - PubMed
-
- Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6:274-9. - PubMed
-
- Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995;4:243-8. - PubMed
-
- Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14:553-65. - PubMed
-
- Burkhart SS, Morgan C. SLAP lesions in the overhead athlete. Orthop Clin North Am. 2001;32:431-41, viii. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
