

Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly
- PMID: 19571280
- PMCID: PMC2917337
- DOI: 10.1056/NEJMoa0810245
Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly
Abstract
Background: It is unknown whether the rate of survival after in-hospital cardiopulmonary resuscitation (CPR) is improving and which characteristics of patients and hospitals predict survival.
Methods: We examined fee-for-service Medicare data from 1992 through 2005 to identify beneficiaries 65 years of age or older who underwent CPR in U.S. hospitals. We examined temporal trends in the incidence of CPR and the rate of survival after CPR, as well as patient- and hospital-level predictors of survival to discharge.
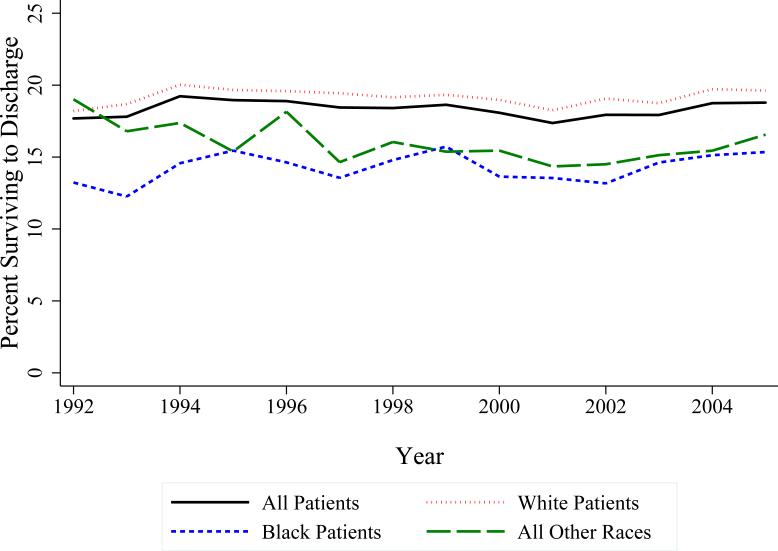
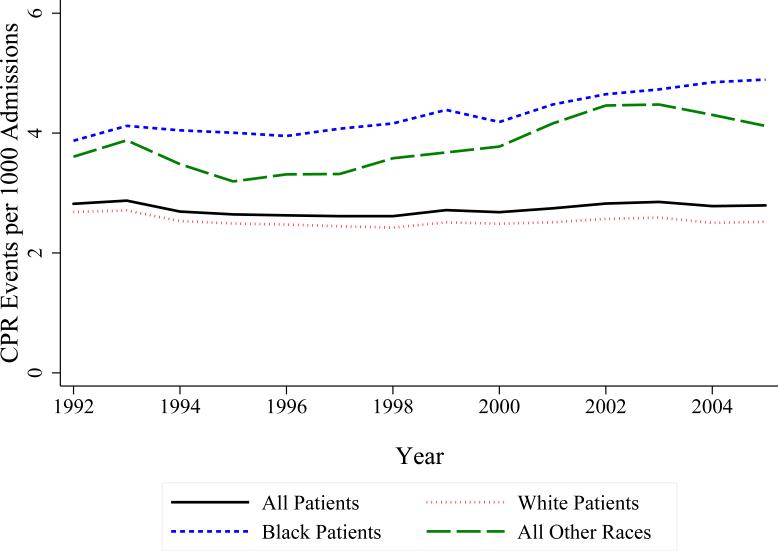
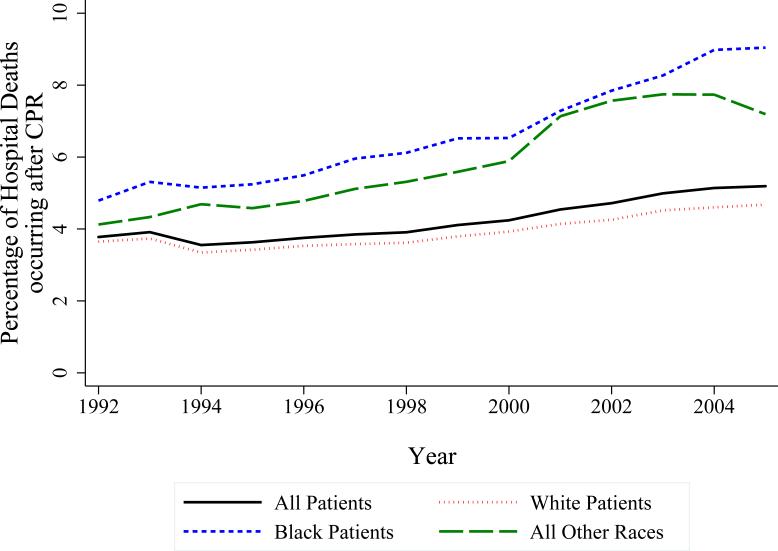
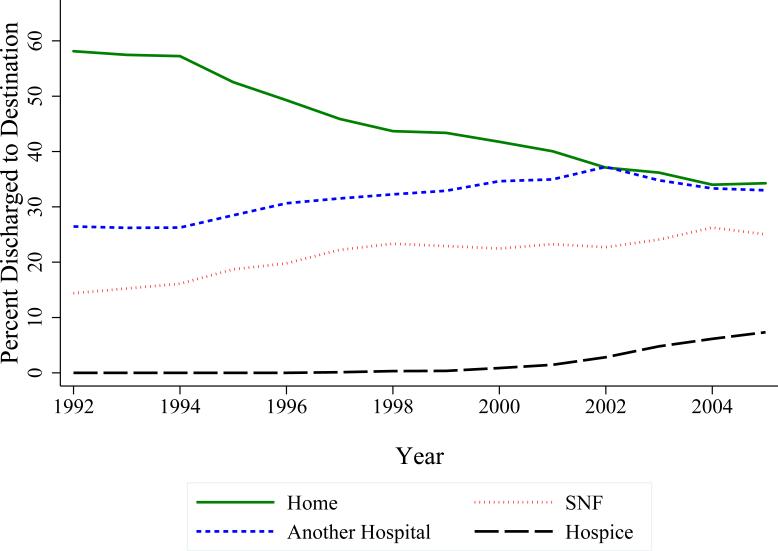
Results: We identified 433,985 patients who underwent in-hospital CPR; 18.3% of these patients (95% confidence interval [CI], 18.2 to 18.5) survived to discharge. The rate of survival did not change substantially during the period from 1992 through 2005. The overall incidence of CPR was 2.73 events per 1000 admissions; the incidence was higher among black and other nonwhite patients. The proportion of patients undergoing in-hospital CPR before death increased over time and was higher for nonwhite patients. The survival rate was lower among patients who were men, were older, had more coexisting illnesses, or were admitted from a skilled-nursing facility. The adjusted odds of survival for black patients were 23.6% lower than those for similar white patients (95% CI, 21.2 to 25.9). The association between race and survival was partially explained by hospital effects: black patients were more likely to undergo CPR in hospitals that have lower rates of post-CPR survival. Among patients surviving in-hospital CPR, the proportion of patients discharged home rather than to a health care facility decreased over time.
Conclusions: Survival after in-hospital CPR did not improve from 1992 through 2005. The proportion of in-hospital deaths preceded by CPR increased, whereas the proportion of survivors discharged home after undergoing CPR decreased. Black race was associated with higher rates of CPR but lower rates of survival after CPR.
2009 Massachusetts Medical Society
Figures
Comment in
-
In-hospital cardiopulmonary resuscitation.N Engl J Med. 2009 Oct 22;361(17):1708; author reply 1708-9. doi: 10.1056/NEJMc091552. N Engl J Med. 2009. PMID: 19846860 No abstract available.
-
In-hospital cardiopulmonary resuscitation.N Engl J Med. 2009 Oct 22;361(17):1708; author reply 1708-9. N Engl J Med. 2009. PMID: 19860012 No abstract available.
References
-
- Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage. Jama. 1960;173:1064–7. - PubMed
-
- Linko E, Koskinen PJ, Siitonen L, Ruosteenoja R. Resuscitation in cardiac arrest. An analysis of 100 successive medical cases. Acta medica Scandinavica. 1967;182:611–20. - PubMed
-
- Nachlas MM, Miller DI. Closed-Chest Cardiac Resuscitation in Patients with Acute Myocardial Infarction. American heart journal. 1965;69:448–59. - PubMed
-
- Eisenberg MS, Bergner L, Hallstrom A. Out-of-hospital cardiac arrest: improved survival with paramedic services. Lancet. 1980;1:812–5. - PubMed
-
- Cobb LA, Fahrenbruch CE, Walsh TR, et al. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out-of-hospital ventricular fibrillation. JAMA. 1999;281:1182–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical