

Non-AIDS-defining deaths and immunodeficiency in the era of combination antiretroviral therapy
- PMID: 19571723
- PMCID: PMC3305466
- DOI: 10.1097/QAD.0b013e32832e9b78
Non-AIDS-defining deaths and immunodeficiency in the era of combination antiretroviral therapy
Abstract
Objective: To assess whether immunodeficiency is associated with the most frequent non-AIDS-defining causes of death in the era of combination antiretroviral therapy (cART).
Design: Observational multicentre cohorts.
Methods: Twenty-three cohorts of adults with estimated dates of human immunodeficiency virus (HIV) seroconversion were considered. Patients were seroconverters followed within the cART era. Measurements were latest CD4, nadir CD4 and time spent with CD4 cell count less than 350 cells/microl. Outcomes were specific causes of death using a standardized classification.
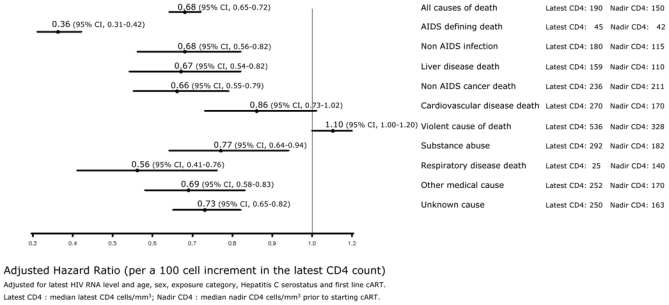
Results: Among 9858 patients (71 230 person-years follow-up), 597 died, 333 (55.7%) from non-AIDS-defining causes. Non-AIDS-defining infection, liver disease, non-AIDS-defining malignancy and cardiovascular disease accounted for 53% of non-AIDS deaths. For each 100 cells/microl increment in the latest CD4 cell count, we found a 64% (95% confidence interval 58-69%) reduction in risk of death from AIDS-defining causes and significant reductions in death from non-AIDS infections (32, 18-44%), end-stage liver disease (33, 18-46%) and non-AIDS malignancies (34, 21-45%). Non-AIDS-defining causes of death were also associated with nadir CD4 while being cART-naive or duration of exposure to immunosuppression. No relationship between risk of death from cardiovascular disease and CD4 cell count was found though there was a raised risk associated with elevated HIV RNA.
Conclusion: In the cART era, the most frequent non-AIDS-defining causes of death are associated with immunodeficiency, only cardiovascular disease was associated with high viral replication. Avoiding profound and mild immunodeficiency, through earlier initiation of cART, may impact on morbidity and mortality of HIV-infected patients.
Conflict of interest statement
Geneviève Chêne has received travel consultancy fees and honoraria from Bohringer Ingelheim, Roche and Gilead Sciences.
Figures
References
-
- Bhaskaran K, Hamouda O, Sannes M, Boufassa F, Johnson AM, Lambert PC, Porter K. Changes in the risk of death after HIV seroconversion compared with mortality in the general population. Jama. 2008;300:51–59. - PubMed
-
- CASCADE Collaboration. Concerted Action on SeroConversion to AIDS and Death in Europe. Survival after introduction of HAART in people with known duration of HIV-1 infection. Lancet. 2000;355:1158–1159. - PubMed
-
- Mocroft A, Brettle R, Kirk O, Blaxhult A, Parkin JM, Antunes F, et al. Changes in the cause of death among HIV positive subjects across Europe: results from the EuroSIDA study. Aids. 2002;16:1663–1671. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. - PubMed
-
- Detels R, Munoz A, McFarlane G, Kingsley LA, Margolick JB, Giorgi J, et al. Effectiveness of potent antiretroviral therapy on time to AIDS and death in men with known HIV infection duration. Multicenter AIDS Cohort Study Investigators. Jama. 1998;280:1497–1503. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
