

Associations between hepatitis B virus mutations and the risk of hepatocellular carcinoma: a meta-analysis
- PMID: 19574418
- PMCID: PMC2720989
- DOI: 10.1093/jnci/djp180
Associations between hepatitis B virus mutations and the risk of hepatocellular carcinoma: a meta-analysis
Abstract
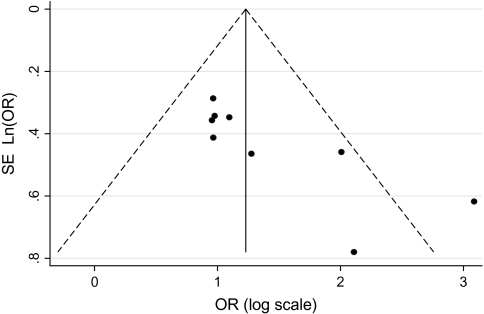
Background: The association between hepatitis B virus (HBV) mutations and hepatocarcinogenesis remains controversial because of conflicting data in the literature. We conducted a meta-analysis of case-control and cohort studies to examine HBV PreS, enhancer II (EnhII), basal core promoter (BCP), and precore mutations in relation to the risk of hepatocellular carcinoma (HCC).
Methods: We searched databases for studies of these associations that were published in English or Chinese up to August 31, 2008. HBV mutation-specific odds ratios and relative risks were pooled by use of a random-effects model and stratified by potential confounders. All statistical tests were two-sided.
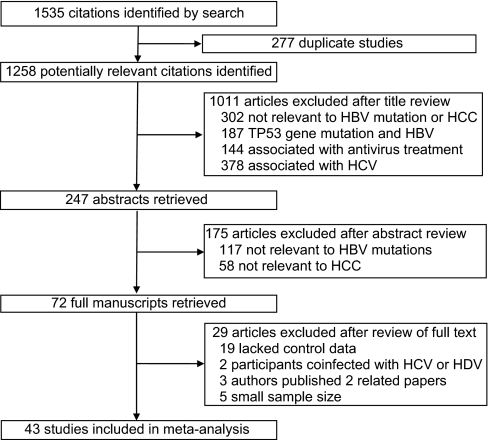
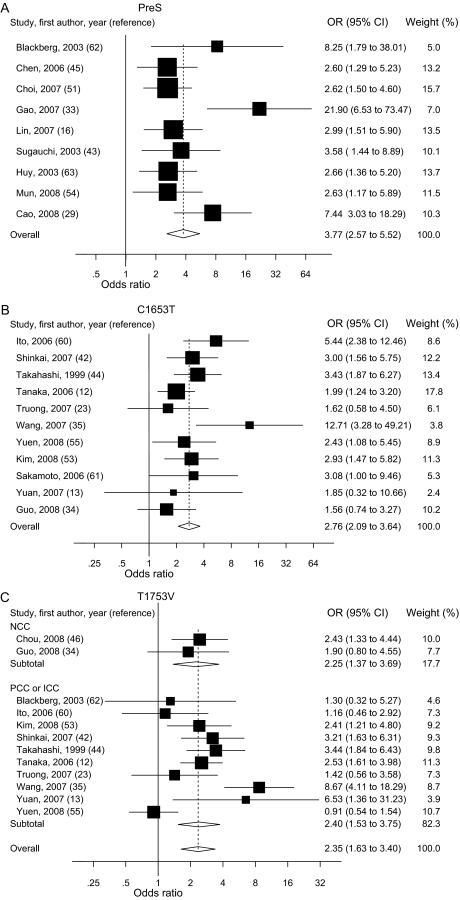
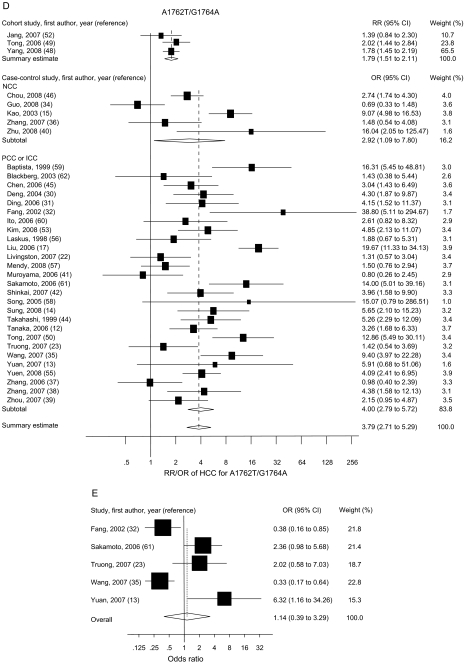
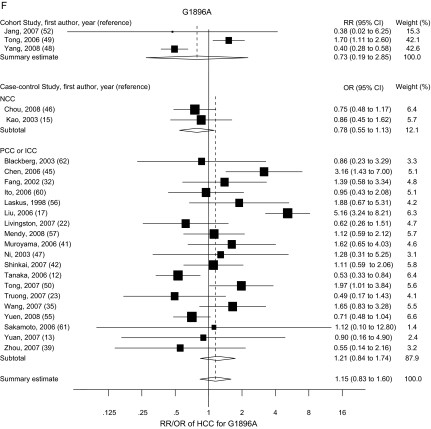
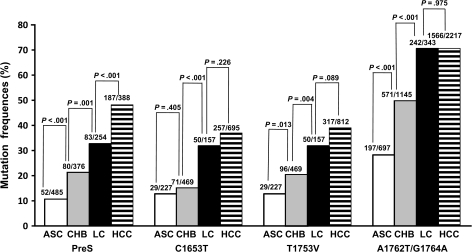
Results: Of the 43 studies included in this meta-analysis, 40 used a case-control design. The 43 studies evaluated a total of 11 582 HBV-infected participants, of whom 2801 had HCC. Statistically significant summary odds ratios of HCC were obtained for any PreS mutation (3.77, 95% confidence interval [CI] = 2.57 to 5.52), C1653T in EnhII (2.76, 95% CI = 2.09 to 3.64), T1753V (2.35, 95% CI = 1.63 to 3.40), and A1762T/G1764A in BCP (3.79, 95% CI = 2.71 to 5.29). PreS mutations were more strongly associated with an increased risk of HCC in subjects who were infected with HBV genotype C than in those who were infected with HBV genotype B, whereas the opposite was true for A1762T/G1764A. C1653T, T1753V, and A1762T/G1764A were more strongly associated with an increased risk of HCC in hepatitis B e antigen (HBeAg)-positive subjects than in HBeAg-negative subjects. PreS mutations, C1653T, T1753V, and A1762T/G1764A accumulated during the progression of chronic HBV infection from the asymptomatic carrier state to HCC (P(trend) < .001 for each mutation). PreS mutations, C1653T, C1653T + T1753V, and A1762T/G1764A-based combinations of mutations had specificities greater than 80% for the prediction of HCC. The precore mutations G1896A and C1858T were not associated with the risk of HCC, regardless of HBeAg status and HBV genotype.
Conclusions: HBV PreS mutations, C1653T, T1753V, and A1762T/G1764A are associated with an increased risk of HCC. These mutations alone and in combination may be predictive for hepatocarcinogenesis.
Figures
References
-
- El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007;132(7):2557–2576. - PubMed
-
- Yu MC, Yuan JM, Govindarajan S, Ross RK. Epidemiology of hepatocellular carcinoma. Can J Gastroenterol. 2000;14(8):703–709. - PubMed
-
- Kay A, Zoulim F. Hepatitis B virus genetic variability and evolution. Virus Res. 2007;127(2):164–176. - PubMed
-
- Yim HJ, Lok AS. Natural history of chronic hepatitis B virus infection: what we knew in 1981 and what we know in 2005. Hepatology. 2006;43(2)(suppl 1):S173–S181. - PubMed
-
- Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295(1):65–73. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
