

Cardiogenic shock without flow-limiting angiographic coronary artery disease: (from the Should We Emergently Revascularize Occluded Coronary Arteries for Cardiogenic Shock Trial and Registry)
- PMID: 19576316
- PMCID: PMC4060258
- DOI: 10.1016/j.amjcard.2009.03.002
Cardiogenic shock without flow-limiting angiographic coronary artery disease: (from the Should We Emergently Revascularize Occluded Coronary Arteries for Cardiogenic Shock Trial and Registry)
Abstract
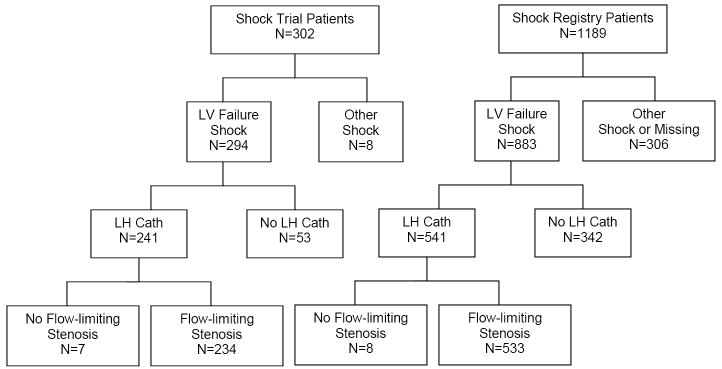
Myocardial infarction often develops when thrombosis occurs at lesions that have not previously been flow limiting. However, the development of cardiogenic shock complicating acute myocardial infarction in such circumstances has received little attention. The characteristics of 15 patients with cardiogenic shock who had no flow-limiting angiographic stenoses were compared with those of 767 patients with > or =1 stenosis who were enrolled in the Should We Emergently Revascularize Occluded Coronary Arteries for Cardiogenic Shock (SHOCK) trial and registry. Compared with patients with > or =1 flow-limiting stenosis, patients with no flow-limiting stenoses were less likely to have pulmonary edema on chest x-ray (29% vs 62%, p = 0.008) and to be white (53% vs 82%, p = 0.011), and they had lower median highest creatine kinase levels (702 vs 2,731 U/L, p = 0.018). For SHOCK trial patients, 1-year survival was 49% for patients with > or =1 flow-limiting stenosis and 71% for those with no flow-limiting stenoses (p = 0.268). In conclusion, patients with cardiogenic shock without flow-limiting stenosis have different characteristics, and potentially disease mechanisms, and they do not require revascularization.
Figures
References
-
- Little WC, Constantinescu M, Applegate RJ, Kutcher MA, Burrows MT, Kahl FR, Santamore WP. Can coronary angiography predict the site of a subsequent myocardial infarction in patients with mild-to-moderate coronary artery disease? Circ. 1988;78:1157–1166. - PubMed
-
- Alpert JS. Fascination with myocardial infarction and normal coronary arteries. Eur Heart J. 2001;22:1364–1366. - PubMed
-
- Pinney SP, Rabbani LE. Myocardial infarction in patients with normal coronary arteries: proposed pathogenesis and predisposing risk factors. J Thromb Thrombolysis. 2001;11:11–17. - PubMed
-
- Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from sudden coronary death: a comprehensive morhpological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol. 2000;20:1262–1267. - PubMed
-
- Goldberg RJ, Samad NA, Yarzebski J, Gurwitz J, Bigelow C, Gore JM. Temporal trends in cardiogenic shock complicating acute myocardial infarction. N Engl J Med. 1999;340:1162–1168. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
