

Comparison between telelaryngoscopy and suspension laryngoscopy in the diagnosis of benign vocal fold lesions
- PMID: 19582343
- PMCID: PMC9445970
- DOI: 10.1016/S1808-8694(15)30147-6
Comparison between telelaryngoscopy and suspension laryngoscopy in the diagnosis of benign vocal fold lesions
Abstract
Proper diagnosis of laryngeal benign lesions still brings doubts among experienced laryngologists, despite current diagnostic progress.
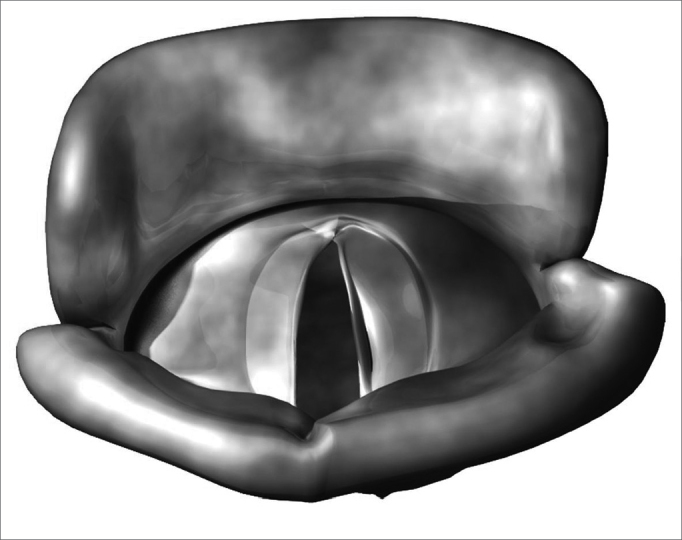
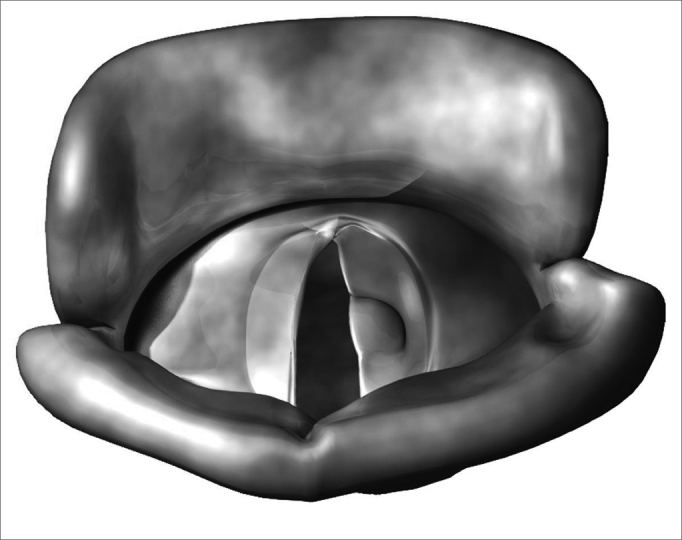
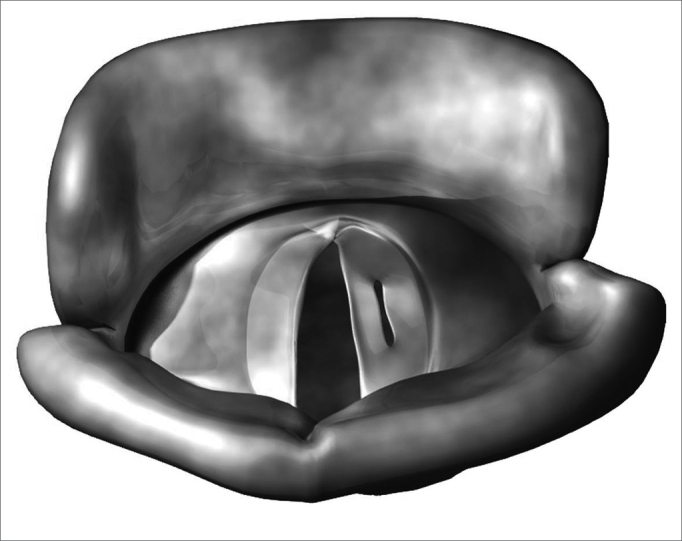
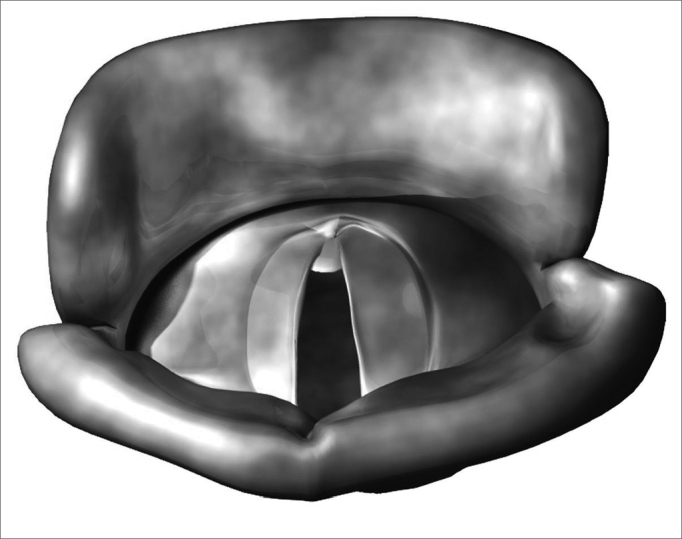
Aim: The goal of this study was to compare telelaryngoscopy (preoperative) with suspension laryngoscopy (intraoperative) on the diagnosis of vocal fold benign lesions.
Materials and methods: We carried out a restrospective study analyzing 79 charts from patients followed up in a University Hospital. In all the charts there was at least diagnostic hypothesis suggested by telelaryngoscopy, which was later on compared to intraoperative findings of suspension laryngoscopy.
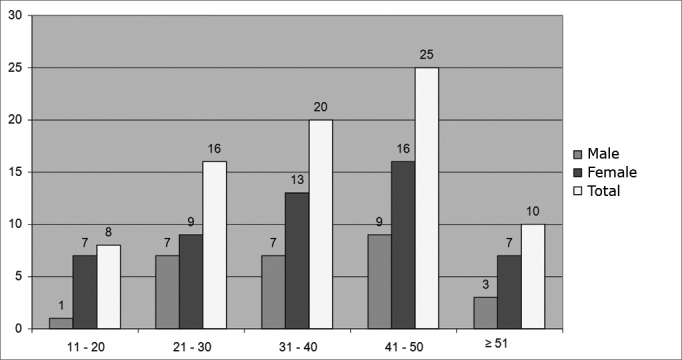
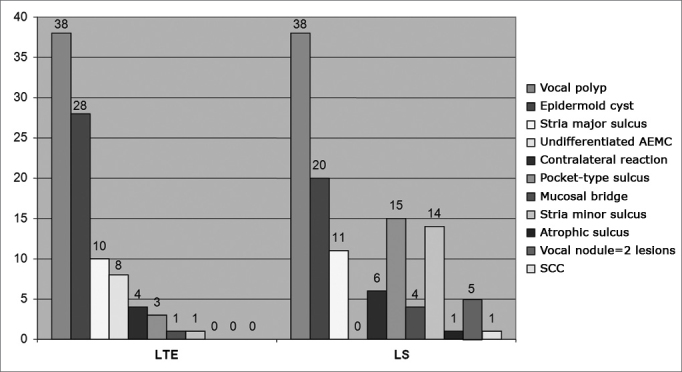
Results: Almost two-thirds of the patients were females, with ages varying between 12 and 66 years (mean of 37 years). Of the 79 patients studied, we diagnosed 95 lesions with telelaryngoscopy and 124 with suspension laryngoscopy. The most frequently found benign lesion was the vocal polyp in both methods. In 64.5% of the cases the diagnosis of the lesions in the outpatient ward was the same as those in the surgical findings.
Conclusion: Laryngologists must be prepared to alter their surgical planning and treatment approaches because of diagnostic changes that may happen during surgery.
Figures
References
-
- Bayle B. Laryngoscopy and laryngoscopes-whos first? The forefathers/four fathers of laryngology. Laryngoscope. 1996;106:939–943. - PubMed
-
- Alberti PW. The history of laryngology: a centennial celebration. Otolaryngol Head Neck Surg. 1996;114:345–354. - PubMed
-
- Cooper RM. Laryngoscopy - its past and future. Can J Anesth. 2004;51:1–5.
-
- Garcia M. Observations on the human voice. Proc Royal Soc Lond. 1885;7:397–410.
-
- Shaw H. Manuel Garcia-A Centenary Tribute. J Laryngol Otol. 1955;69:342–346. - PubMed
Uncited Reference
-
- Bouchayer M, Cornut G. Les sulcus glottidis:Notions nouvelles apportées par la microchirurgie laryngée:a propos de 31 cas. Cah Otorhinolaryngol. 1978;13:769–777.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
