

Bladder neck contracture after retropubic radical prostatectomy: incidence and risk factors from a large single-surgeon experience
- PMID: 19583720
- PMCID: PMC3173809
- DOI: 10.1111/j.1464-410X.2009.08700.x
Bladder neck contracture after retropubic radical prostatectomy: incidence and risk factors from a large single-surgeon experience
Abstract
Objective: To examine a large, single-surgeon series of patients with prostate cancer who underwent retropubic radical prostatectomy (RRP) for men with postoperative bladder neck contractures (BNCs).
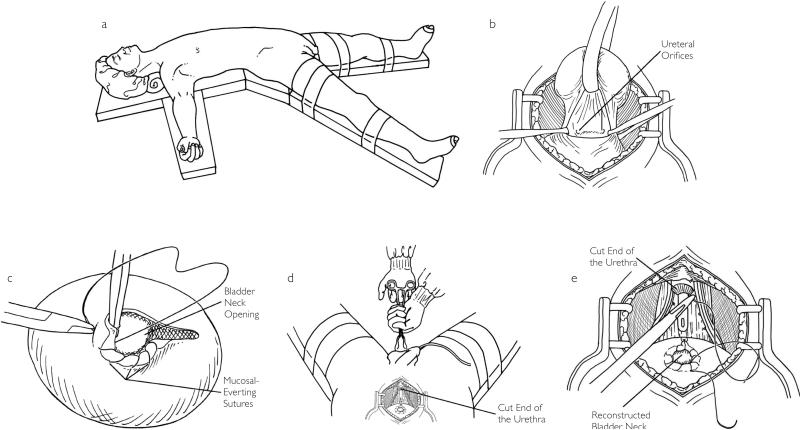
Patients and methods: From 1983 to 2007, 4132 men underwent RRP for prostate cancer by one surgeon. All patients had BN reconstruction with mucosal eversion. The bladder to membranous urethral anastomosis was made using six 2/0 chromic catgut sutures over an 18 F Foley catheter. The catheter was left in place for 10 days. Data from these men is stored in a prospective database, which was reviewed in this study for men with BNCs after RRP. Men with BNCs were compared with all other men in the series to determine risk factors for BNC development.
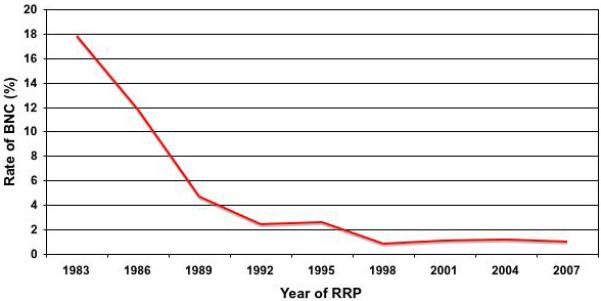
Results: Overall, BNCs developed in 110 patients (2.5%). Examining our last 500 patients there was a contemporary BNC rate of <1%. The median (range) follow-up was 44 (12-233) months. Tumour characteristics were similar in the men with BNCs and those with no BNCs, and the rates of organ-confined disease were also similar (65% vs 70%, P = 0.27). Men with BNCs had higher median preoperative prostate-specific antigen (PSA) levels (6.7 vs 5.7 mg/dL; P = 0.009) and were more likely to have PSA failure after RRP (30% vs 16%, P < 0.001). On multivariate analysis, non-nerve sparing (P = 0.003) and a surgical date before 1992 (P < 0.001) were significant predictors of BNC. Patients with BNCs had lower potency rates (49% vs 63%, P < 0.003) and continence rates (88% vs 94%, P = 0.07) at the 18-month follow-up.
Conclusions: BNCs are rare, occurring in <1% in our modern series. The important surgical factors in preventing BNCs are to avoid closing the BN too tightly and attaining good apposition of the BN with the urethral stump with a watertight closure. BNCs are more common with non-nerve-sparing surgery and early in a surgeon's experience.
Figures
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Park R, Martin S, Goldberg JD, Lepor H. Anastomotic strictures following radical prostatectomy. insights into incidence, effectiveness of intervention, effect on continence, and factors predisposing to occurrence. Urology. 2001;57:742–6. - PubMed
-
- Anger JT, Raj GV, Delvecchio FC, Webster GD. Anastomotic contracture and incontinence after radical prostatectomy: a graded approach to management. J Urol. 2005;173:1143–6. - PubMed
-
- Herr HW. Quality of life of incontinent men after radical prostatectomy. J Urol. 1994;151:652–4. - PubMed
-
- Kao TC, Cruess DF, Garner D, et al. Multicenter patient self-reporting questionnaire on impotence, incontinence and stricture after radical prostatectomy. J Urol. 2000;163:858–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
