

The relation between the incidence of hypernatremia and mortality in patients with severe traumatic brain injury
- PMID: 19583864
- PMCID: PMC2750153
- DOI: 10.1186/cc7953
The relation between the incidence of hypernatremia and mortality in patients with severe traumatic brain injury
Abstract
Introduction: The study was aimed at verifying whether the occurrence of hypernatremia during the intensive care unit (ICU) stay increases the risk of death in patients with severe traumatic brain injury (TBI). We performed a retrospective study on a prospectively collected database including all patients consecutively admitted over a 3-year period with a diagnosis of TBI (post-resuscitation Glasgow Coma Score < or = 8) to a general/neurotrauma ICU of a university hospital, providing critical care services in a catchment area of about 1,200,000 inhabitants.
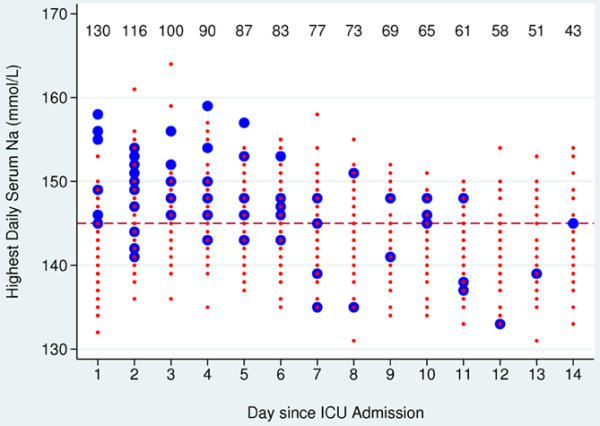
Methods: Demographic, clinical, and ICU laboratory data were prospectively collected; serum sodium was assessed an average of three times per day. Hypernatremia was defined as two daily values of serum sodium above 145 mmol/l. The major outcome was death in the ICU after 14 days. Cox proportional-hazards regression models were used, with time-dependent variates designed to reflect exposure over time during the ICU stay: hypernatremia, desmopressin acetate (DDAVP) administration as a surrogate marker for the presence of central diabetes insipidus, and urinary output. The same models were adjusted for potential confounding factors.
Results: We included in the study 130 TBI patients (mean age 52 years (standard deviation 23); males 74%; median Glasgow Coma Score 3 (range 3 to 8); mean Simplified Acute Physiology Score II 50 (standard deviation 15)); all were mechanically ventilated; 35 (26.9%) died within 14 days after ICU admission. Hypernatremia was detected in 51.5% of the patients and in 15.9% of the 1,103 patient-day ICU follow-up. In most instances hypernatremia was mild (mean 150 mmol/l, interquartile range 148 to 152). The occurrence of hypernatremia was highest (P = 0.003) in patients with suspected central diabetes insipidus (25/130, 19.2%), a condition that was associated with increased severity of brain injury and ICU mortality. After adjustment for the baseline risk, the incidence of hypernatremia over the course of the ICU stay was significantly related with increased mortality (hazard ratio 3.00 (95% confidence interval: 1.34 to 6.51; P = 0.003)). However, DDAVP use modified this relation (P = 0.06), hypernatremia providing no additional prognostic information in the instances of suspected central diabetes insipidus.
Conclusions: Mild hypernatremia is associated with an increased risk of death in patients with severe TBI. In a proportion of the patients the association between hypernatremia and death is accounted for by the presence of central diabetes insipidus.
Figures
Comment in
-
Sodium and brain injury: do we know what we are doing?Crit Care. 2009;13(5):184. doi: 10.1186/cc8014. Epub 2009 Sep 3. Crit Care. 2009. PMID: 19804616 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
