

Timing of levothyroxine administration affects serum thyrotropin concentration
- PMID: 19584184
- PMCID: PMC2758731
- DOI: 10.1210/jc.2009-0860
Timing of levothyroxine administration affects serum thyrotropin concentration
Abstract
Context: Patients treated with levothyroxine typically ingest it in a fasting state to prevent food impairing its absorption. The serum thyrotropin concentration is the therapeutic index of levothyroxine action.
Objective: The study objective was to determine the effect of the timing of levothyroxine administration in relationship to food on serum thyrotropin levels.
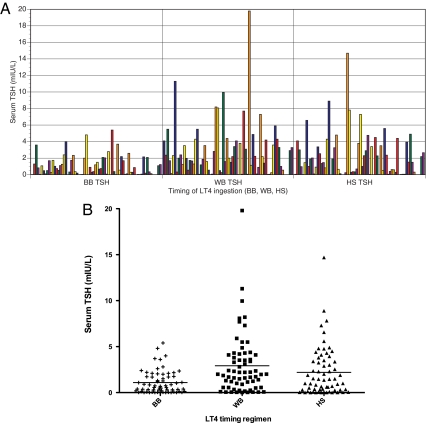
Design: Participants were randomized to one of six sequences, each consisting of three 8-wk regimens in a three-period crossover design. These regimens were in a fasting state, at bedtime, and with breakfast. The concentrations of TSH, free T(4), and total T(3) during each of the three timing regimens were documented. The primary outcome was the difference between serum TSH concentrations under fasting conditions compared with concentrations during the other 8-wk regimens.
Setting: The study was conducted in an academic medical center.
Participants: Study participants were receiving levothyroxine for treatment of hypothyroidism or thyroid cancer.
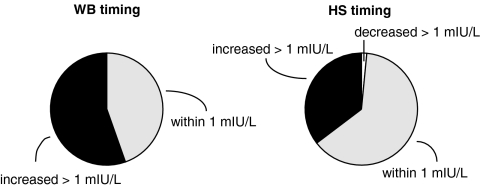
Results: Sixty-five patients completed the study. The mean thyrotropin concentration was 1.06 +/- 1.23 mIU/liter when levothyroxine was administered in the fasting state. When levothyroxine was taken with breakfast, the serum thyrotropin concentration was significantly higher (2.93 +/- 3.29 mIU/liter). When levothyroxine was taken at bedtime, the serum TSH concentration was also significantly higher (2.19 +/- 2.66 mIU/liter).
Conclusion: Nonfasting regimens of levothyroxine administration are associated with higher and more variable serum TSH concentrations. If a specific serum TSH goal is desired, thereby avoiding iatrogenic subclinical thyroid disease, then fasting ingestion of levothyroxine ensures that TSH concentrations remain within the narrowest target range.
Figures
References
-
- Wenzel KW, Kirschsieper HE 1977 Aspects of the absorption of oral l-thyroxine in normal man. Metabolism 26:1–8 - PubMed
-
- Lamson MJ, Pamplin CL, Rolleri RL, Klein I 2004 Quantitation of a substantial reduction in levothyroxine (T4) absorption by food. Thyroid 14:876
-
- Hays MT 2007 Parenteral thyroxine administration. Thyroid 17:127–129 - PubMed
-
- Wenzel KW 1986 [Optimization of levothyroxine treatment. Dosage dependence on the existing parenchymal mass, age, body weight and fasting intake]. Dtsch Med Wochenschr 111:1356–1362 - PubMed
-
- Fish LH, Schwartz HL, Cavanaugh J, Steffes MW, Bantle JP, Oppenheimer JH 1987 Replacement dose, metabolism, and bioavailability of levothyroxine in the treatment of hypothyroidism. Role of triiodothyronine in pituitary feedback in humans. N Engl J Med 316:764–770 - PubMed
