

Racial disparities in cancer survival among randomized clinical trials patients of the Southwest Oncology Group
- PMID: 19584328
- PMCID: PMC2724852
- DOI: 10.1093/jnci/djp175
Racial disparities in cancer survival among randomized clinical trials patients of the Southwest Oncology Group
Abstract
Background: Racial disparities in cancer outcomes have been observed in several malignancies. However, it is unclear if survival differences persist after adjusting for clinical, demographic, and treatment variables. Our objective was to determine whether racial disparities in survival exist among patients enrolled in consecutive trials conducted by the Southwest Oncology Group (SWOG).
Methods: We identified 19 457 adult cancer patients (6676 with breast, 2699 with lung, 1244 with colon, 1429 with ovarian, and 1843 with prostate cancers; 1291 with lymphoma; 2067 with leukemia; and 2208 with multiple myeloma) who were treated on 35 SWOG randomized phase III clinical trials from October 1, 1974, through November 29, 2001. Patients were grouped according to studies of diseases with similar histology and stage. Cox regression was used to evaluate the association between race and overall survival within each disease site grouping, controlling for available prognostic factors plus education and income, which are surrogates for socioeconomic status. Median and ten-year overall survival estimates were derived by the Kaplan-Meier method. All statistical tests were two-sided.
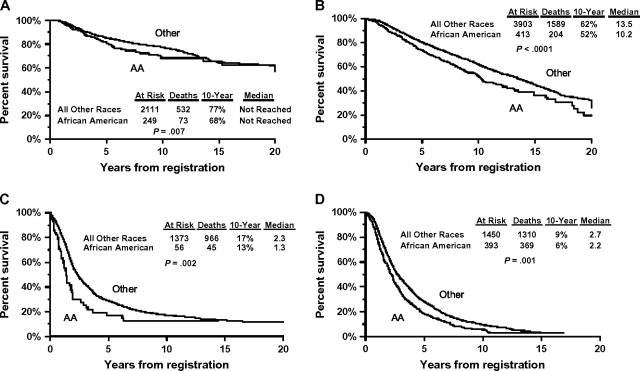
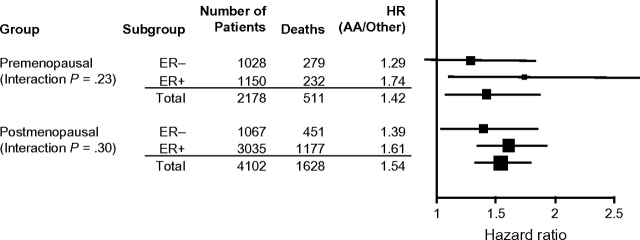
Results: Of 19 457 patients registered, 2308 (11.9%, range = 3.9%-21.6%) were African American. After adjustment for prognostic factors, African American race was associated with increased mortality in patients with early-stage premenopausal breast cancer (hazard ratio [HR] for death = 1.41, 95% confidence interval [CI] = 1.10 to 1.82; P = .007), early-stage postmenopausal breast cancer (HR for death = 1.49, 95% CI = 1.28 to 1.73; P < .001), advanced-stage ovarian cancer (HR for death = 1.61, 95% CI = 1.18 to 2.18; P = .002), and advanced-stage prostate cancer (HR for death = 1.21, 95% CI = 1.08 to 1.37; P = .001). No statistically significant association between race and survival for lung cancer, colon cancer, lymphoma, leukemia, or myeloma was observed. Additional adjustments for socioeconomic status did not substantially change these observations. Ten-year (and median) overall survival rates for African American vs all other patients were 68% (not reached) vs 77% (not reached), respectively, for early-stage, premenopausal breast cancer; 52% (10.2 years) vs 62% (13.5 years) for early-stage, postmenopausal breast cancer; 13% (1.3 years) vs 17% (2.3 years) for advanced ovarian cancer; and 6% (2.2 years) vs 9% (2.7 years) for advanced prostate cancer.
Conclusions: African American patients with sex-specific cancers had worse survival than white patients, despite enrollment on phase III SWOG trials with uniform stage, treatment, and follow-up.
Figures
Comment in
-
Is race really a negative prognostic factor for cancer?J Natl Cancer Inst. 2009 Jul 15;101(14):970-1. doi: 10.1093/jnci/djp185. Epub 2009 Jun 30. J Natl Cancer Inst. 2009. PMID: 19567421 No abstract available.
-
Re: Racial disparities in cancer survival among randomized clinical trials of the Southwest Oncology Group.J Natl Cancer Inst. 2010 Feb 24;102(4):277; author reply 280-2. doi: 10.1093/jnci/djp510. Epub 2010 Jan 14. J Natl Cancer Inst. 2010. PMID: 20075363 Free PMC article. No abstract available.
-
Re: Racial disparities in cancer survival among randomized clinical trials of the Southwest Oncology Group.J Natl Cancer Inst. 2010 Feb 24;102(4):278-9; author reply 280-2. doi: 10.1093/jnci/djp508. Epub 2010 Jan 14. J Natl Cancer Inst. 2010. PMID: 20075364 Free PMC article. No abstract available.
-
Re: Racial disparities in cancer survival among randomized clinical trials of the Southwest Oncology Group.J Natl Cancer Inst. 2010 Feb 24;102(4):277-8; author reply 280-2. doi: 10.1093/jnci/djp507. Epub 2010 Jan 14. J Natl Cancer Inst. 2010. PMID: 20075366 No abstract available.
-
Re: Racial disparities in cancer survival among randomized clinical trials of the Southwest Oncology Group.J Natl Cancer Inst. 2010 Feb 24;102(4):279-80; author reply 280-2. doi: 10.1093/jnci/djp505. Epub 2010 Jan 14. J Natl Cancer Inst. 2010. PMID: 20075368 No abstract available.
-
Re: Racial disparities in cancer survival among randomized clinical trials of the Southwest Oncology Group.J Natl Cancer Inst. 2010 Feb 24;102(4):280; author reply 280-2. doi: 10.1093/jnci/djp506. Epub 2010 Jan 14. J Natl Cancer Inst. 2010. PMID: 20075371 No abstract available.
References
-
- Edwards BK, Brown ML, Wingo PA, et al. Annual report to the nation on the status of cancer, 1975–2002, featuring population-based trends in cancer treatment. J Natl Cancer Inst. 2005;97(19):1407–1427. - PubMed
-
- Jemal A, Clegg LX, Ward E, et al. Annual report to the nation on the status of cancer, 1975–2001, with a special feature regarding survival. Cancer. 2004;101(1):3–27. - PubMed
-
- Freeman HP, Muth BJ, Kerner JF. Expanding access to cancer screening and clinical follow-up among the medically underserved. Cancer Pract. 1995;3(1):19–30. - PubMed
-
- Underwood SM. Reducing the burden of cancer borne by African Americans: if not now, when? Cancer Epidemiol Biomarkers Prev. 2003;12(3):270s–276s. - PubMed
-
- Dignam JJ, Colangelo L, Tian W, et al. Outcomes among African-Americans and Caucasians in colon cancer adjuvant therapy trials: findings from the National Surgical Adjuvant Breast and Bowel Project. J Natl Cancer Inst. 1999;91(22):1933–1940. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
