

An independent external validation and evaluation of QRISK cardiovascular risk prediction: a prospective open cohort study
- PMID: 19584409
- PMCID: PMC2714681
- DOI: 10.1136/bmj.b2584
An independent external validation and evaluation of QRISK cardiovascular risk prediction: a prospective open cohort study
Abstract
Objective: To independently evaluate the performance of the QRISK score for predicting 10 year risk of cardiovascular disease in an independent UK cohort of patients from general practice and compare the performance with Framingham equations.
Design: Prospective open cohort study.
Setting: 274 practices from England and Wales contributing to the THIN database.
Participants: 1.07 million patients, registered between 1 January 1995 and 1 April 2006, aged 35-74 years (5.4 million person years) with 43 990 cardiovascular events.
Main outcome measures: First diagnosis of cardiovascular disease (myocardial infarction, coronary heart disease, stroke, and transient ischaemic attack) recorded in general practice records.
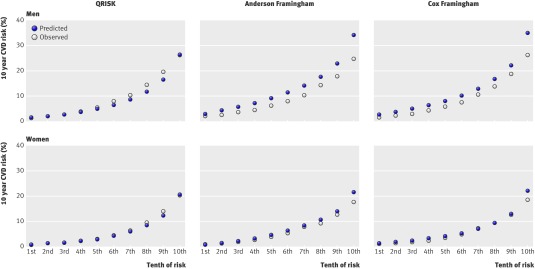
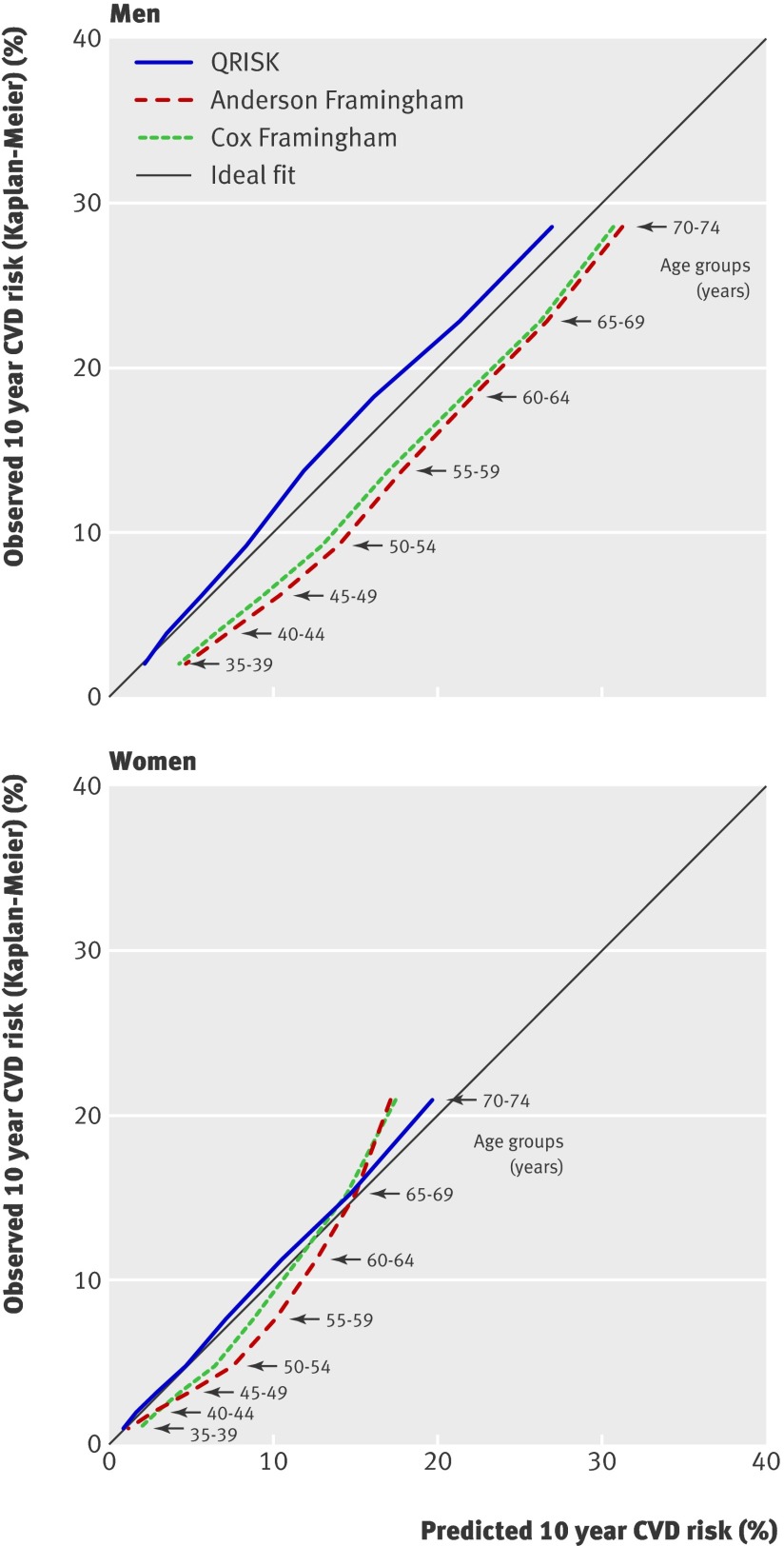
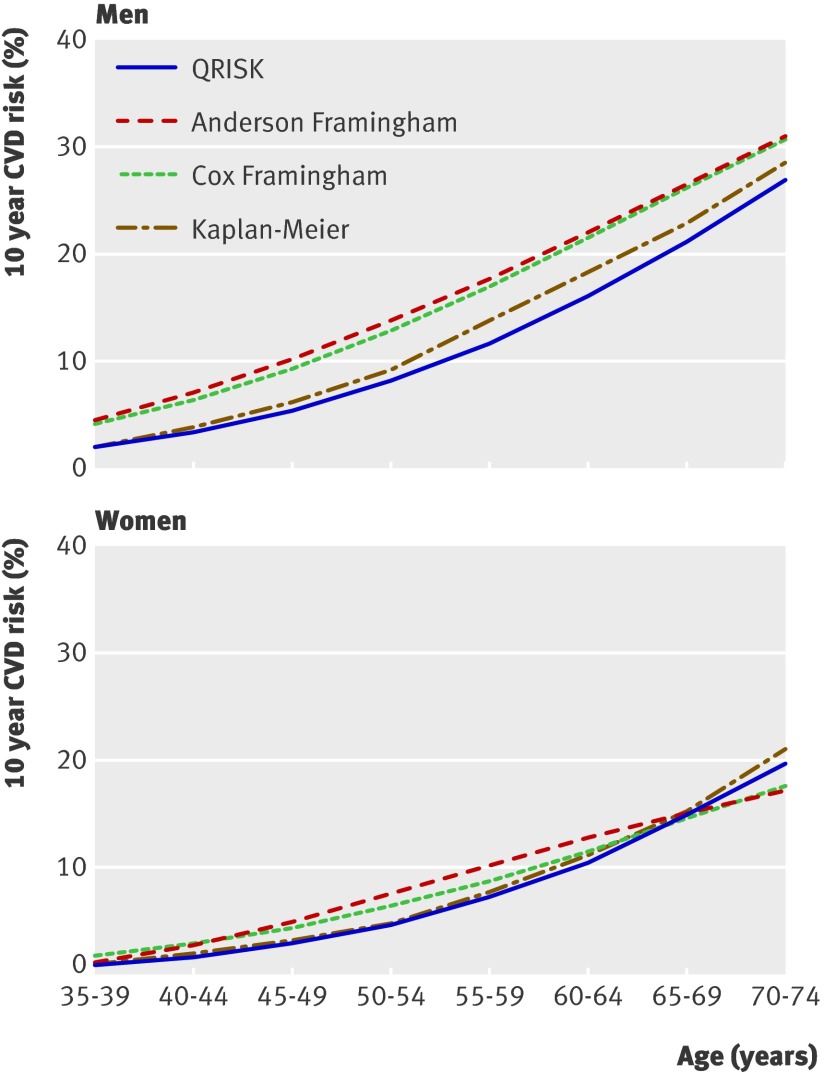
Results: This independent validation indicated that QRISK offers an improved performance in predicting the 10 year risk of cardiovascular disease in a large cohort of UK patients over the Anderson Framingham equation. Discrimination and calibration statistics were better with QRISK. QRISK explained 32% of the variation in men and 37% in women, compared with 27% and 31% respectively for Anderson Framingham. QRISK underpredicted risk by 13% for men and 10% for women, whereas Anderson Framingham overpredicted risk by 32% for men and 10% for women. In total, 85 010 (8%) of patients would be reclassified from high risk (>or=20%) with Anderson Framingham to low risk with QRISK, with an observed 10 year cardiovascular disease risk of 17.5% (95% confidence interval 16.9% to 18.1%) for men and 16.8% (15.7% to 18.0%) for women. The incidence rate of cardiovascular disease events among men was 30.5 per 1000 person years (95% confidence interval 29.9 to 31.2) in high risk patients identified with QRISK and 23.7 per 1000 person years (23.2 to 24.1) in high risk patients identified with Anderson Framingham. Similarly, the incidence rate of cardiovascular disease events among women was 26.7 per 1000 person years (25.8 to 27.7) in high risk patients identified with QRISK compared with 22.2 per 1000 person years (21.4 to 23.0) in high risk patients identified with Anderson Framingham.
Conclusions: The QRISK cardiovascular disease risk equation offers an improvement over the long established Anderson Framingham equation in terms of identifying a high risk population for cardiovascular disease in the United Kingdom. QRISK underestimates 10 year cardiovascular disease risk, but the magnitude of underprediction is smaller than the overprediction with Anderson Framingham.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
QRISK or Framingham for predicting cardiovascular risk?BMJ. 2009 Jul 7;339:b2673. doi: 10.1136/bmj.b2673. BMJ. 2009. PMID: 19584410 No abstract available.
-
QRISK validation and evaluation. QRISK may be less useful.BMJ. 2009 Sep 1;339:b3485. doi: 10.1136/bmj.b3485. BMJ. 2009. PMID: 19723713 No abstract available.
-
QRISK validation and evaluation. Bespoke cohort studies needed.BMJ. 2009 Sep 1;339:b3512. doi: 10.1136/bmj.b3512. BMJ. 2009. PMID: 19723720 No abstract available.
-
ASSIGN, QRISK, and validation.BMJ. 2009 Sep 1;339:b3514. doi: 10.1136/bmj.b3514. BMJ. 2009. PMID: 19723721 No abstract available.
References
-
- Moons KGM, Royston P, Vergouwe Y, Grobbee DE, Altman DG. Prognosis and prognostic research: what, why, and how? BMJ 2009;338:b375. - PubMed
-
- Wyatt JC, Altman DG. Commentary: Prognostic models: clinical useful or quickly forgotten? BMJ 1995;311:1539-41.
-
- Altman DG, Vergouwe Y, Royston P, Moons KGM. Prognosis and prognostic research: validating a prognostic model. BMJ 2009;338:b605. - PubMed
-
- Altman DG, Royston P. What do we mean by validating a prognostic model? Stat Med 2000;19:453-73. - PubMed
-
- Bleeker SE, Moll HA, Steyerberg EW, Donders ART, Derksen-Lubsen G, Grobbee DE, et al. External validation is necessary in prediction research: a clinical example. J Clin Epidemiol 2003;56:826-32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous