

Review
doi: 10.1080/09273940903108544.
Primary intraocular lymphoma: diagnosis and differential diagnosis
Affiliations
- PMID: 19585354
- PMCID: PMC2924171
- DOI: 10.1080/09273940903108544
Item in Clipboard
Review
Primary intraocular lymphoma: diagnosis and differential diagnosis
Ocul Immunol Inflamm.
2009 May-Jun.
Abstract
Diagnosis of PIOL can be challenging. It requires a high degree of clinical suspicion and differential diagnosis includes infectious and non-infectious etiologies particularly the common masquaraders sarcoidosis, tuberculosis, viral retinitis and syphilis. The definitive diagnosis depends on demonstration of malignant lymphoma cells in ocular specimens or CSF. Ocular specimen could include vitreous, aqueous or chorioretinal biopsy. Ocular pathologist should be consulted prior to the diagnostic procedure to help handle and process the specimen appropriately. In addition to cytology, flow cytometry, immunohistochemistry, molecular analysis and cytokines may be used as adjuncts in facilitating the diagnosis.
Figures
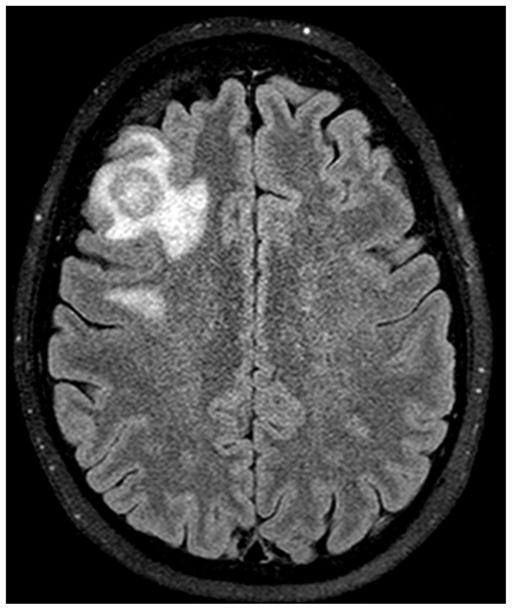
CNS involvement in a patient with primary intraocular lymphoma. Note the enhancing mass slightly larger than 1.5 cm in the right middle frontal gyrus surrounded by modest amount of vasogenic edema.
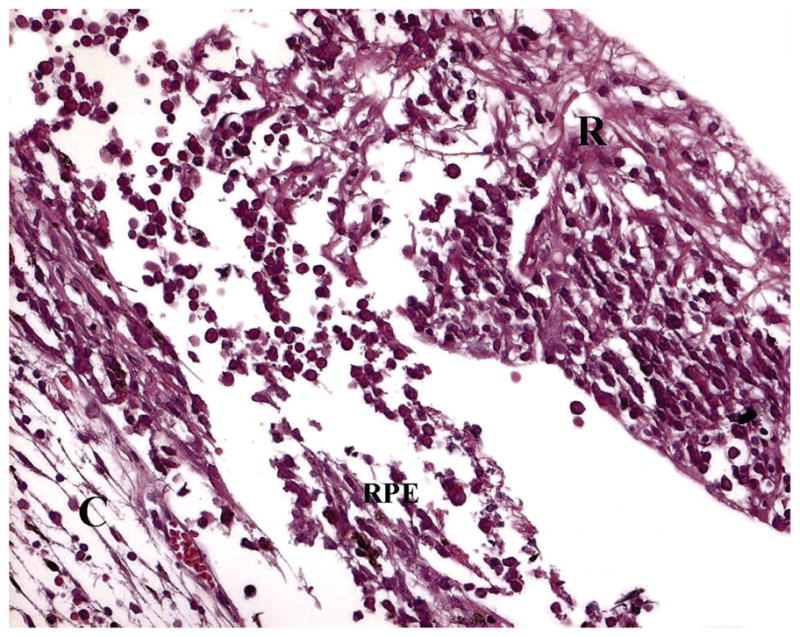
Lymphoma cells located both in the sub-RPE space and invading into the retina (H&E) (C: choroid, RPE: retinal pigment epithelium, R: retina).
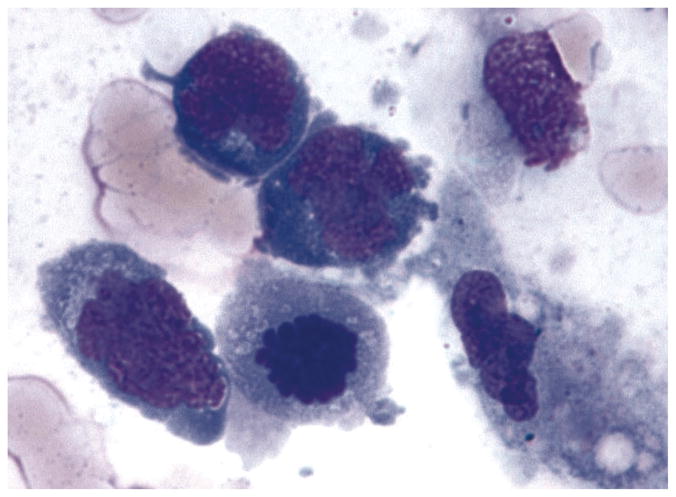
Photomicropgraph showing lymphoma cells from the vitreous of a patient with PIOL. Note the lymphoma cells are large with scanty basophilic cytoplasm and large hyper-segmented nuclei and prominent nucleoli (Giemsa).
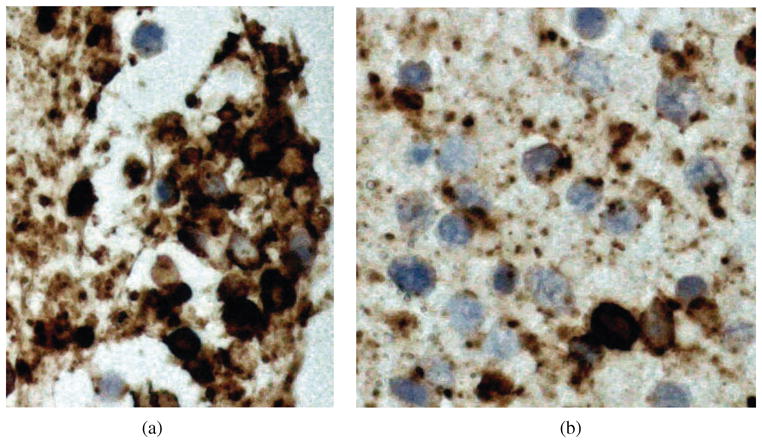
Figure 4A and B. Immunohistochemistry of lymphoma cells can help differentiate B- and T-cell lymphomas. Majority of PIOL are monoclonal B-cell lymphomas that stain positively for B-cell markers, such as CD20 (A), however there may be some reactive T-cells that stain positively for T-cell markers, such as CD3 (B).

Micro-dissection and PCR of a lymphoma cell from vitreous reveals IgH gene rearrangement using the third complementarity-determining region (CDR3) as primer.
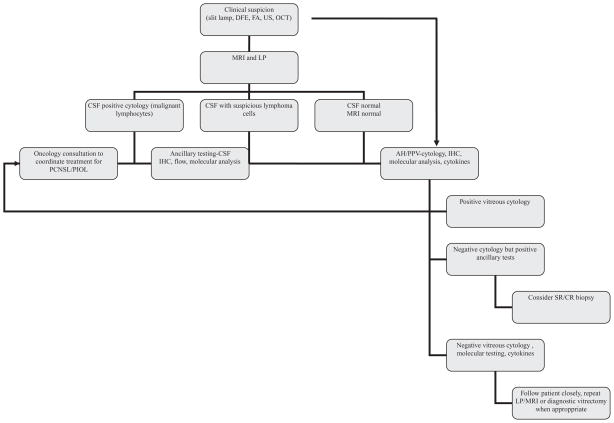
Flowchart representing diagnostic approach by the authors. (DFE: dilated fundus exam, FA: fluorescein angiography, US: ultrasound, OCT: optical coherence tomography, IHC: immunohistochemistry, AH: aqueous humor, PPV: pars plana vitrectomy, CSF: cerebrospinal fluid, MRI: magnetic resonance imaging).
References
-
- Chan CC, Gonzalez JA. Primary Intraocular Lymphoma. Hackensack, NJ: World Scientific Publishing Co. Pte. Ltd; 2007.
-
- Coupland SE, Damato B. Understanding intraocular lymphoma. Clin Experiment Opthalmol. 2008;26(6):564–578. - PubMed
-
- Barr CC, Green WR, Payne JW, et al. Intraocular reticulum-cell sarcoma: clinicopathologic study of four cases and review of the literature. Surv Ophthalmol. 1975;19(4):224–239. - PubMed
-
- Kaplan HJ, Meredith TA, Aaberg TM, et al. Reclassification of intraocular reticulum cell sarcoma (histiocytic lymphoma). Immunologic characterization of vitreous cells. Arch Ophthalmol. 1980;98:707–710. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources