

Pregabalin for acute and chronic pain in adults
- PMID: 19588419
- PMCID: PMC4167351
- DOI: 10.1002/14651858.CD007076.pub2
Pregabalin for acute and chronic pain in adults
Update in
-
Pregabalin for neuropathic pain in adults.Cochrane Database Syst Rev. 2019 Jan 23;1(1):CD007076. doi: 10.1002/14651858.CD007076.pub3. Cochrane Database Syst Rev. 2019. PMID: 30673120 Free PMC article.
Abstract
Background: Antiepileptic drugs have been used in pain management since the 1960s. Pregabalin is a recently developed antiepileptic drug also used in management of chronic neuropathic pain conditions.
Objectives: To assess analgesic efficacy and associated adverse events of pregabalin in acute and chronic pain.
Search strategy: We searched MEDLINE, EMBASE, and CENTRAL to May 2009 for randomised controlled trials (RCTs). Additional studies were identified from the reference lists of retrieved papers and on-line clinical trial databases.
Selection criteria: Randomised, double blind trials reporting on the analgesic effect of pregabalin, with subjective pain assessment by the patient as either the primary or a secondary outcome.
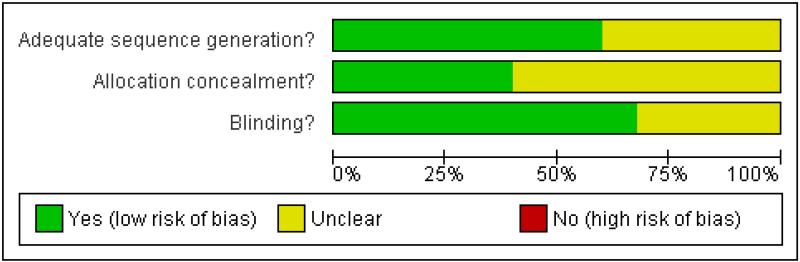
Data collection and analysis: Two independent review authors extracted data and assessed trial quality. Numbers-needed-to-treat-to-benefit (NNTs) were calculated, where possible, from dichotomous data for effectiveness, adverse events and study withdrawals.
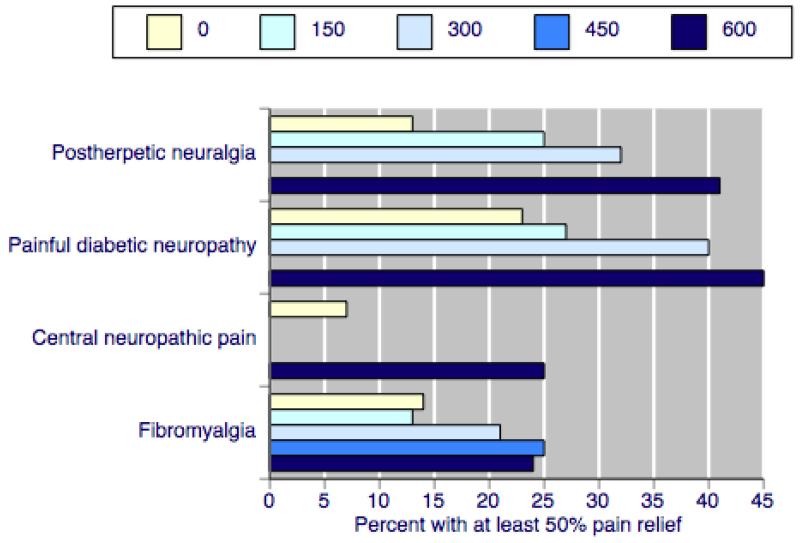
Main results: There was no clear evidence of beneficial effects of pregabalin in established acute postoperative pain. No studies evaluated pregabalin in chronic nociceptive pain, like arthritis.Pregabalin at doses of 300 mg, 450 mg, and 600 mg daily was effective in patients with postherpetic neuralgia, painful diabetic neuropathy, central neuropathic pain, and fibromyalgia (19 studies, 7003 participants). Pregabalin at 150 mg daily was generally ineffective. Efficacy was demonstrated for dichotomous outcomes equating to moderate or substantial pain relief, alongside lower rates for lack of efficacy discontinuations with increasing dose. The best (lowest) NNT for each condition for at least 50% pain relief over baseline (substantial benefit) for 600 mg pregabalin daily compared with placebo were 3.9 (95% confidence interval 3.1 to 5.1) for postherpetic neuralgia, 5.0 (4.0 to 6.6) for painful diabetic neuropathy, 5.6 (3.5 to 14) for central neuropathic pain, and 11 (7.1 to 21) for fibromyalgia.With 600 mg pregabalin daily somnolence typically occurred in 15% to 25% and dizziness occurred in 27% to 46%. Treatment was discontinued due to adverse events in 18 to 28%. The proportion of participants reporting at least one adverse event was not affected by dose, nor was the number with a serious adverse event, which was not more than with placebo.Higher rates of substantial benefit were found in postherpetic neuralgia and painful diabetic neuropathy than in central neuropathic pain and fibromyalgia. For moderate and substantial benefit on any outcome NNTs for the former were generally six and below for 300 mg and 600 mg daily; for fibromyalgia NNTs were much higher, and generally seven and above.
Authors' conclusions: Pregabalin has proven efficacy in neuropathic pain conditions and fibromyalgia. A minority of patients will have substantial benefit with pregabalin, and more will have moderate benefit. Many will have no or trivial benefit, or will discontinue because of adverse events. Individualisation of treatment is needed to maximise pain relief and minimise adverse events. There is no evidence to support the use of pregabalin in acute pain scenarios.
Figures

Comment in
-
ACP Journal Club. Review: pregabalin reduces chronic neuropathic pain in adults.Ann Intern Med. 2009 Dec 15;151(12):JC6-7. doi: 10.7326/0003-4819-151-12-200912150-02007. Ann Intern Med. 2009. PMID: 20008756 No abstract available.
References
References to studies included in this review
-
- Anon A randomized double-blind, placebo-controlled, parallel-group, multi-center trial of pregabalin versus placebo in the treatment of neuropathic pain associated with diabetic peripheral neuropathy. PhRMA Clinical Study Synopsis 19 December 2007
-
- Anon A 14-week, randomized, double-blind, placebo-controlled trial of pregabalin twice daily in patients with fibromyalgia. PhRMA Web Synopsis 7–March–2008
-
- Anon A 13-week, randomized, double-blind, multicenter, placebo-controlled study to evaluate efficacy and safety of pregabalin (CI-1008) in the treatment of postherpetic neuralgia. PhRMA Web Synopsis 1–September–2008
-
- Agarwal A, Gautam S, Gupta D, Agarwal S, Singh PK, Singh U. Evaluation of a single preoperative dose of pregabalin for attenuation of postoperative pain after laparoscopic cholecystectomy. British Journal of Anaesthetics. 2008;101(5):700–4. [DOI: 10.1093/bja/aen244] - PubMed
References to studies excluded from this review
-
- Reuben SS, Buvanendran A, Kroin JS, Raghunathan K. The analgesic efficacy of celecoxib, pregabalin, and their combination for spinal fusion surgery. Anesthesia and Analgesia. 2006;103(5):1271–7. [DOI: 10.1213/01.ane.0000237279.08847.2d] - PubMed
Additional references
-
- Attal N, Cruccu G, Haanpaa M, Hansson P, Jensen TS, EFNS Task Force et al. EFNS guidelines on pharmacological treatment of neuropathic pain. European Journal of Neurology. 2006;13:1153–69. [DOI: 10.1111/j.1468-1331.2006.01511.x] - PubMed
-
- Dahl JB, Mathiesen O, Miniche S. ’Protective premedication’: an option with gabapentin and related drugs? A review of gabapentin and pregabalin in the treatment of post-operative pain. Acta Anaesthesiologica Scandinavica. 2004;48(9):1130–6. [DOI: 10.1111/j.1399-6576.2004.00484.x] - PubMed
-
- Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. The Journal of Pain. 2008;9(2):105–21. [DOI: 10.1016/j.jpain.2007.09.005] - PubMed
-
- Edwards JE, McQuay HJ, Moore RA, Collins SL. Reporting of adverse effects in clinical trials should be improved: lessons from acute postoperative pain. Journal of Pain and Symptom Management. 1999;18(6):427–37. [DOI: 10.1016/S0885-3924(99)00093-7] - PubMed
-
- Edwards JE, McQuay HJ, Moore RA. Efficacy and safety of valdecoxib for treatment of osteoarthritis and rheumatoid arthritis: systematic review of randomised controlled trials. Pain. 2004;111(3):286–96. [DOI: 10.1016/j.pain.2004.07.004] - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical