

Addition of long-acting beta-agonists to inhaled corticosteroids for chronic asthma in children
- PMID: 19588447
- PMCID: PMC4167878
- DOI: 10.1002/14651858.CD007949
Addition of long-acting beta-agonists to inhaled corticosteroids for chronic asthma in children
Update in
-
Addition of long-acting beta2-agonists to inhaled corticosteroids for chronic asthma in children.Cochrane Database Syst Rev. 2015 Nov 24;2015(11):CD007949. doi: 10.1002/14651858.CD007949.pub2. Cochrane Database Syst Rev. 2015. PMID: 26594816 Free PMC article.
Abstract
Background: Long-acting ss(2)- agonists (LABA) in combination with inhaled corticosteroids (ICS) are increasingly prescribed in asthmatic children.
Objectives: To compare the safety and benefit of adding LABA to ICS with the same or an increased dose of ICS in children with persistent asthma.
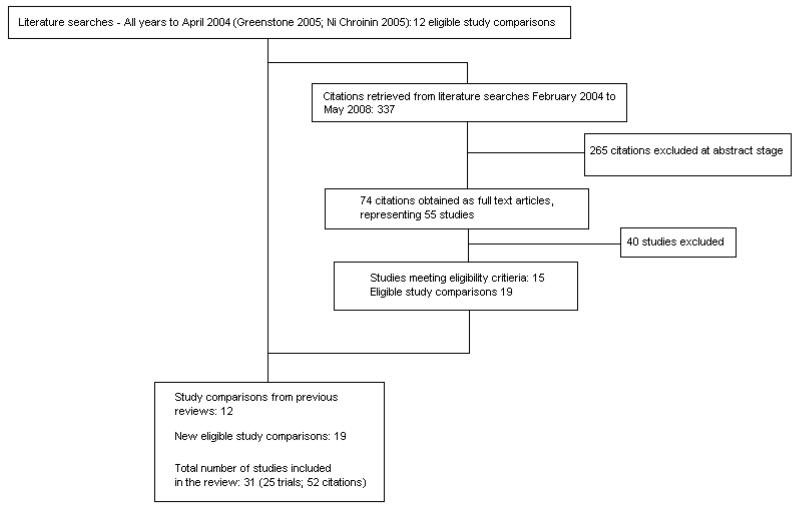
Search strategy: We searched the Cochrane Airways Group Asthma Trials Register (May 2008).
Selection criteria: We included randomised controlled trials testing the combination of LABA and ICS versus the same or an increased dose of ICS for minimum of at least 28 days in children and adolescents with asthma. The main outcome was the rate of exacerbations requiring rescue oral steroids. Secondary outcomes included pulmonary function, symptoms, adverse events, and withdrawals.
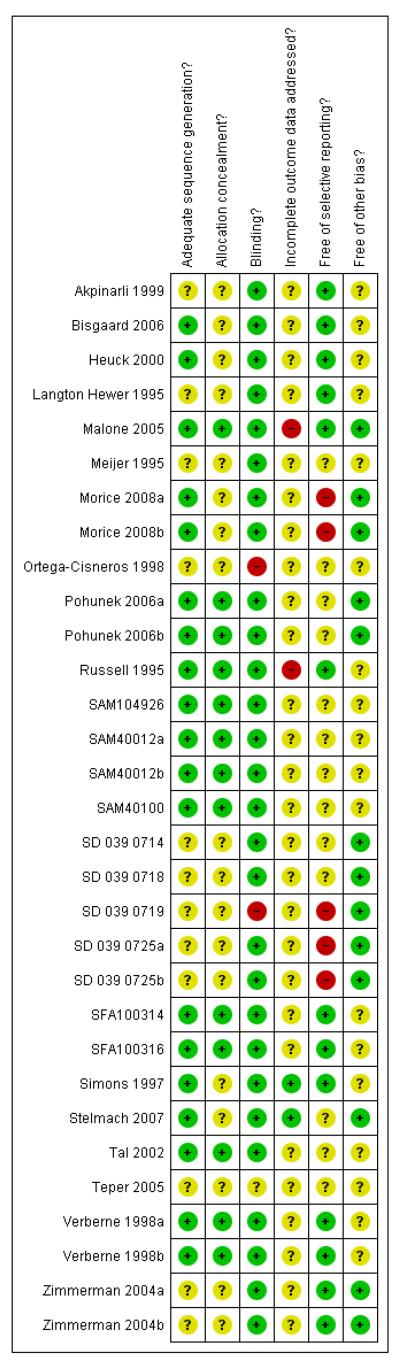
Data collection and analysis: Studies were assessed independently by two review authors for methodological quality and data extraction. Confirmation was obtained from the trialists when possible.
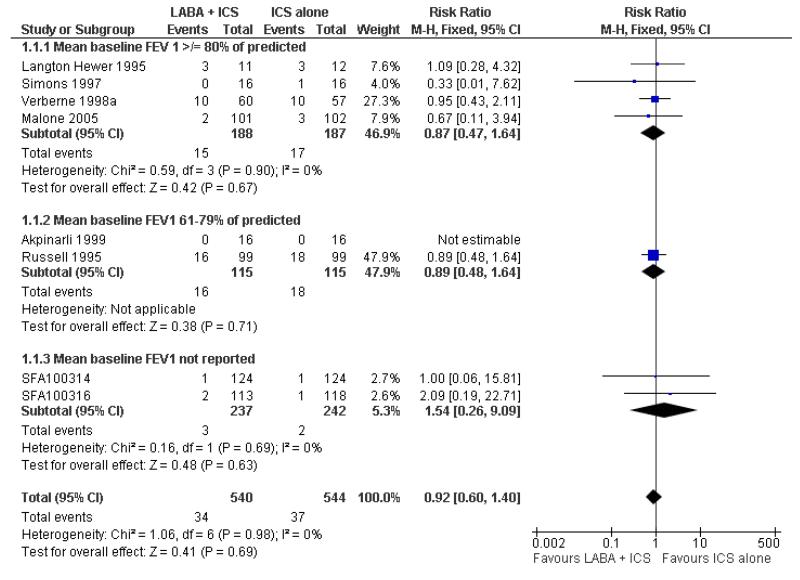
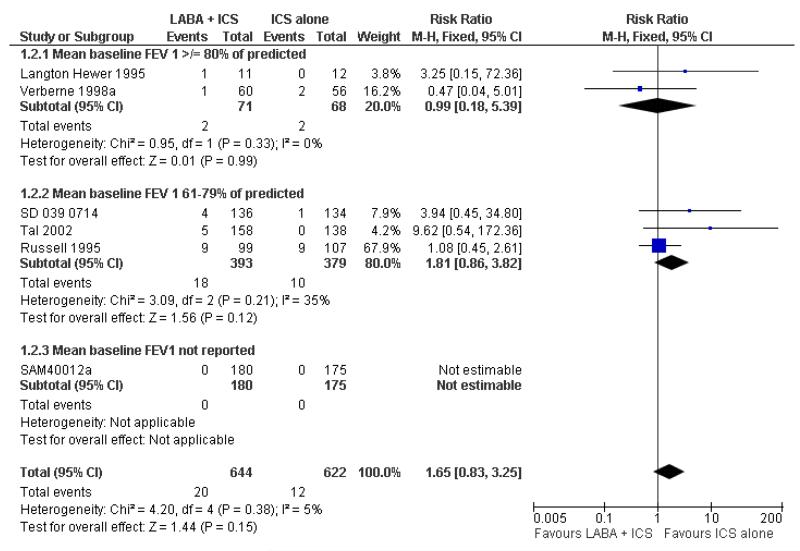
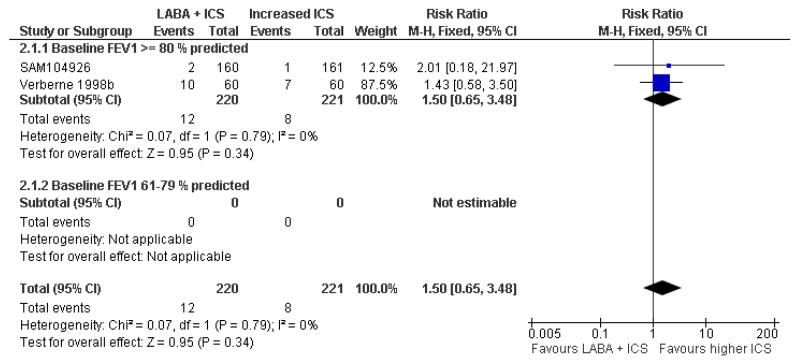
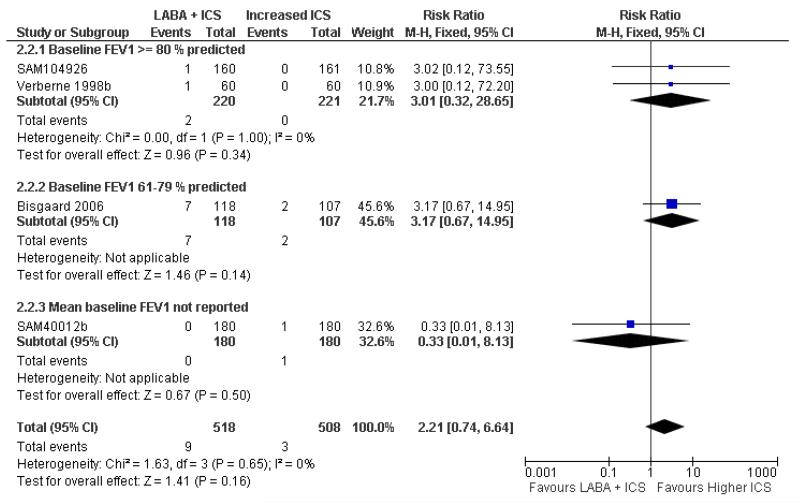
Main results: A total of 25 trials representing 31 control-intervention comparisons were included in the review randomising 5572 children. Most of the participants were inadequately controlled on current ICS dose. We assessed the addition of LABA to the same dose of ICS and to an increased dose of ICS:(1) The addition of LABA to ICS was compared to same dose ICS, namely 400 mcg/day of beclomethasone or less in 16 of the 24 studies. The mean age of participants was 10 years and males accounted for 64% of the study populations. The mean FEV(1) at baseline was 80% of predicted or above in 10 studies; FEV(1) 61% to 79% of predicted in eight studies; and unreported in the remaining study. Participants were inadequately controlled before randomisation in all but seven studies. Compared to ICS alone, the addition of LABA to ICS was not associated with a significant reduction in exacerbations requiring oral steroids (seven studies, RR 0.92 95% CI 0.60 to 1.40). Compared to ICS alone, there was a significantly greater improvement in FEV1 with the addition of LABA (nine studies; 0.08 Litres, 95% CI 0.06 to 0.11) but no statistically significant group differences in symptom-free days, hospital admission, quality of life, use of reliever medication, and adverse events. Withdrawals occurred significantly less frequently with the addition of LABA.(2) A total of seven studies assessed the addition of LABA to ICS therapy compared with an increased dose of ICS randomising 1021 children. The mean age of participants was 8 years with 67% of males. The baseline mean FEV(1) was 80% of predicted or above in 2 of the 3 studies reporting this characteristic. All trials enrolled participants who were inadequately controlled on a baseline dose equivalent to 400 mcg/day of beclomethasone or less. There was no group significant difference in the risk of an exacerbation requiring oral steroids with the combination of LABA and ICS compared to a double dose of ICS (two studies, RR 1.5 95% CI 0.65 to 3.48). The increased risk of hospital admission with combination therapy was also not statistically significant (RR 2.21 95% CI 0.74 to 6.64). Compared to double dose ICS, use of LABA was associated with a significantly greater improvement in morning PEF (four studies; MD 7.55 L/min 95% CI: 3.57 to 11.53) and evening PEF L/min (three studies, MD 5.5 L/min; 95% CI 1.21 to 9.79), but there were insufficient data to aggregate data on FEV(1), symptoms, rescue reliever use, and quality of life. There was no statistically significant difference in the overall risk of all cause withdrawals (five studies; RR 0.71; 95% CI 0.42 to 1.20. There was no group difference in the risk of overall adverse effects detected. Short term growth was significantly greater in children treated with combination therapy compared to double dose ICS (two studies: MD 1.2 cm/year; 95% CI 0.72 to 1.7).
Authors' conclusions: In children with persistent asthma, the addition of LABA to ICS was not associated with a significant reduction in the rate of exacerbations requiring systemic steroids, but was superior for improving lung function compared to the same dose of ICS. Similarly, compared to a double dose ICS, the combination of LABA and ICS did not significantly increase the risk of exacerbations requiring oral steroids, but was associated with a significantly greater improvement in PEF and growth. The possibility of an increased risk of rescue oral steroids and hospital admission with LABA therapy needs to be further examined.
Figures
References
References to studies included in this review
-
- Barnes PJ, O’Byrne PM, Rodriguez-Roisin R, Runnerstrom E, Sandstrom T, Svensson K, Tattersfield A. Oxis and Pulmicort turbuhaler in the management of asthma OPTIMA international study group. Treatment of mild persistent asthma with low doses of inhaled Budesonide alone or in combination with Formoterol. Thorax. 2000;55(Suppl 3):A4.
-
- Barnes PJ, O’Byrne PM, Rodriguez-Roisin R, Runnerstrom E, Sandstrom T, Svensson K, Tattersfield A. Treatment of mild persistent asthma with low doses of inhaled budesonide alone or in combination with formoterol. For the Oxis and Pulmicort Turbuhaler in the Management of Asthma (OPTIMA) international study group. Thorax. 2000;55(Suppl 3):s5.
-
- Bisgaard H, Hultquist C. Budesonide/formoterol for maintenance and as needed - a new approach to asthma management in children [Abstract] European Respiratory Journal. 2005;26(Suppl 49) Abstract No. 1060.
-
-
*
- Bisgaard H, Le Roux P, Bjamer D, Dymek A, Vermeulen JH, Hultquist C. Budesonide/formoterol maintenance plus reliever therapy - a new strategy in pediatric asthma. Chest. 2006;130(6) - PubMed
-
References to studies excluded from this review
-
- Aldington S, Williams M, Weatherall M, Beasley R. Duration of action of the salmeterol/fluticasone combination inhaler administered in the evening: A randomized controlled trial in childhood asthma. Respirology. 2006;11(5):638–42. - PubMed
-
- Aubier M, Pieters WR, Schlosser NJ, Steinmetz KO. Salmeterol/fluticasone propionate (50/500 mug) in combination in a Diskus(TM) inhaler (Seretide(TM)) is effective and safe in the treatment of steroid-dependent asthma. Respiratory Medicine. 1999;93(12):876–84. - PubMed
-
- Bergmann KC, Lindemann L, Braun R, Steinkamp G. Salmeterol/fluticasone propionate (50/250 microg) combination is superior to double dose fluticasone (500 microg) for the treatment of symptomatic moderate asthma. Swiss Medical Weekly. 2004;134(3-4):50–8. - PubMed
-
- Borker R, Emmett A, Jhingran P, Rickard K, Dorinsky P. Determining economic feasibility of fluticasone propionate-salmeterol vs montelukast in the treatment of persistent asthma using a net benefit approach and cost-effectiveness acceptability curves. Annals of Allergy, Asthma, & Immunology. 2005;95(2):181–9. - PubMed
-
- Boulet LP, Roberts J, Watson EG. Efficacy of salmeterol/fluticasone propionate MDI versus higher dose fluticasone propionate in adolescent and adult asthmatics uncontrolled on fluticasone propionate alone [Abstract] European Respiratory Journal. 2003;22(Suppl 45) Abstract No: [P2799]
Additional references
-
- Adams NP, Bestall JC, Lasserson TJ, Jones P, Cates CJ. Fluticasone versus placebo for chronic asthma in adults and children. Cochrane Database of Systematic Reviews. 2008;(4) DOI: 10.1002/14651858.CD003135.Pub4. - PubMed
-
- Bateman E, Nelson H, Bousquet J, Kral K, Sutton L, Ortega H, et al. [accessed 5th June 2008];Meta-analysis: Effects of adding salmeterol to inhaled corticosteroids on serious asthma-related events. 2008 149(1) www.annals.org. Epub. - PubMed
-
- Bisgaard H. Effect of long-acting ß2-agonists on exacerbation rates of asthma in children. Pediatric Pulmonology. 2003;36:391–8. - PubMed
References to other published versions of this review
-
- Greenstone IR, Ni Chroinin MN, Masse V, Danish A, Magdalinos H, Zhang X, Ducharme FM. Combination of inhaled long-acting beta2-agonists and inhaled steroids versus higher dose of inhaled steroids in children and adults with persistent asthma. Cochrane Database of Systematic Reviews. 2005;(4) DOI: 10.1002/14651858.CD005533. - PubMed
-
- Ni Chroinin M, Greenstone IR, Danish A, Magdolinos H, Masse V, Zhang X, Ducharme FM. Long-acting beta2-agonists versus placebo in addition to inhaled corticosteroids in children and adults with chronic asthma. Cochrane Database of Systematic Reviews. 2005;(4) DOI: 10.1002/14651858.CD005535. - PubMed
-
-
*Indicates the major publication for the study
-
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical