

Hyperactivated B cells in human inflammatory bowel disease
- PMID: 19589946
- PMCID: PMC2796625
- DOI: 10.1189/jlb.0309203
Hyperactivated B cells in human inflammatory bowel disease
Abstract
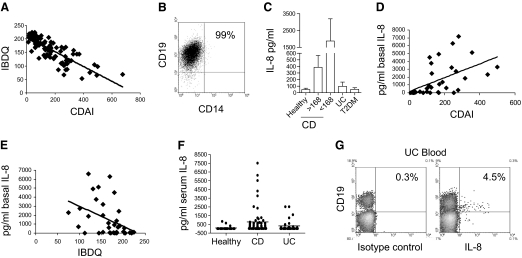
IBD is characterized by a chronic, dysregulated immune response to intestinal bacteria. Past work has focused on the role of T cells and myeloid cells in mediating chronic gastrointestinal and systemic inflammation. Here, we show that circulating and tissue B cells from CD patients demonstrate elevated basal levels of activation. CD patient B cells express surface TLR2, spontaneously secrete high levels of IL-8, and contain increased ex vivo levels of phosphorylated signaling proteins. CD clinical activity correlates directly with B cell expression of IL-8 and TLR2, suggesting a positive relationship between these B cell inflammatory mediators and disease pathogenesis. In contrast, B cells from UC patients express TLR2 but generally do not demonstrate spontaneous IL-8 secretion; however, significant IL-8 production is inducible via TLR2 stimulation. Furthermore, UC clinical activity correlates inversely with levels of circulating TLR2+ B cells, which is opposite to the association observed in CD. In conclusion, TLR2+ B cells are associated with clinical measures of disease activity and differentially associated with CD- and UC-specific patterns of inflammatory mediators, suggesting a formerly unappreciated role of B cells in the pathogenesis of IBD.
Figures





References
-
- Loftus E V., Jr Clinical epidemiology of inflammatory bowel disease: incidence, prevalence, and environmental influences. Gastroenterology. 2004;126:1504–1517. - PubMed
-
- Baumgart D C, Carding S R. Inflammatory bowel disease: cause and immunobiology. Lancet. 2007;369:1627–1640. - PubMed
-
- Rakoff-Nahoum S, Medzhitov R. Role of Toll-like receptors in tissue repair and tumorigenesis. Biochemistry (Mosc) 2008;73:555–561. - PubMed
-
- Cario E, Gerken G, Podolsky D K. Toll-like receptor 2 controls mucosal inflammation by regulating epithelial barrier function. Gastroenterology. 2007;132:1359–1374. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
