

Quality improvement in depression care in the Netherlands: the Depression Breakthrough Collaborative. A quality improvement report
- PMID: 19590610
- PMCID: PMC2707591
- DOI: 10.5334/ijic.314
Quality improvement in depression care in the Netherlands: the Depression Breakthrough Collaborative. A quality improvement report
Abstract
Background: Improving the healthcare for patients with depression is a priority health policy across the world. Roughly, two major problems can be identified in daily practice: (1) the content of care is often not completely consistent with recommendations in guidelines and (2) the organization of care is not always integrated and delivered by multidisciplinary teams.
Aim: To describe the content and preliminary results of a quality improvement project in primary care, aiming at improving the uptake of clinical depression guidelines in daily practice as well as the collaboration between different mental health professionals.
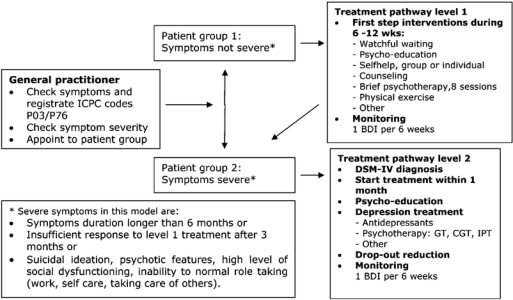
Method: A Depression Breakthrough Collaborative was initiated from December 2006 until March 2008. The activities included the development and implementation of a stepped care depression model, a care pathway with two levels of treatment intensity: a first step treatment level for patients with non-severe depression (brief or mild depressive symptoms) and a second step level for patients with severe depression. Twelve months data were measured by the teams in terms of one outcome and several process indicators. Qualitative data were gathered by the national project team with a semi-structured questionnaire amongst the local team coordinators.
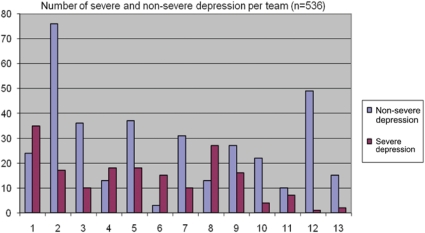
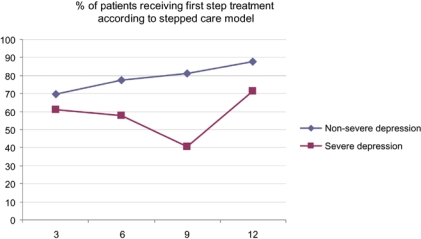
Results: Thirteen multidisciplinary teams participated in the project. In total 101 health professionals were involved, and 536 patients were diagnosed. Overall 356 patients (66%) were considered non-severely depressed and 180 (34%) patients showed severe symptoms. The mean percentage of non-severe patients treated according to the stepped care model was 78%, and 57% for the severely depressed patient group. The proportion of non-severely depressed patients receiving a first step treatment according to the stepped care model, improved during the project, this was not the case for the severely depressed patients. The teams were able to monitor depression symptoms to a reasonable extent during a period of 6 months. Within 3 months, 28% of monitored patients had recovered, meaning a Beck Depression Inventory (BDI) score of 10 and lower, and another 27% recovered between 3 and 6 months.
Conclusions and discussion: A stepped care approach seems acceptable and feasible in primary care, introducing different levels of care for different patient groups. Future implementation projects should pay special attention to the quality of care for severely depressed patients. Although the Depression Breakthrough Collaborative introduced new treatment concepts in primary and specialty care, the change capacity of the method remains unclear. Thorough data gathering is needed to judge the real value of these intensive improvement projects.
Keywords: Breakthrough Collaborative; care pathway; depression; multidisciplinary teams; quality improvement; stepped care.
Figures
Similar articles
-
Implementing a stepped-care approach in primary care: results of a qualitative study.Implement Sci. 2012 Jan 31;7:8. doi: 10.1186/1748-5908-7-8. Implement Sci. 2012. PMID: 22293362 Free PMC article.
-
Stepped collaborative depression care: primary care results before and after implementation of a stepped collaborative depression programme.Fam Pract. 2014 Apr;31(2):180-92. doi: 10.1093/fampra/cmt072. Epub 2013 Nov 25. Fam Pract. 2014. PMID: 24277384
-
Stepped care for depression is easy to recommend, but harder to implement: results of an explorative study within primary care in the Netherlands.BMC Fam Pract. 2014 Jan 9;15:5. doi: 10.1186/1471-2296-15-5. BMC Fam Pract. 2014. PMID: 24400701 Free PMC article.
-
Does shared care help in the treatment of depression?Psychiatr Danub. 2010 Nov;22 Suppl 1:S18-22. Psychiatr Danub. 2010. PMID: 21057395 Review.
-
Nonsomatic treatment of depression.Child Adolesc Psychiatr Clin N Am. 2002 Jul;11(3):579-93. doi: 10.1016/s1056-4993(02)00009-3. Child Adolesc Psychiatr Clin N Am. 2002. PMID: 12222084 Review.
Cited by
-
Relations between mental health team characteristics and work role performance.PLoS One. 2017 Oct 9;12(10):e0185451. doi: 10.1371/journal.pone.0185451. eCollection 2017. PLoS One. 2017. PMID: 28991923 Free PMC article.
-
Implementing a stepped-care approach in primary care: results of a qualitative study.Implement Sci. 2012 Jan 31;7:8. doi: 10.1186/1748-5908-7-8. Implement Sci. 2012. PMID: 22293362 Free PMC article.
-
Introducing hepatitis C virus healthcare pathways in addiction care in the Netherlands with a Breakthrough project: a mixed method study.Harm Reduct J. 2019 Jul 15;16(1):45. doi: 10.1186/s12954-019-0316-4. Harm Reduct J. 2019. PMID: 31307470 Free PMC article.
-
Supportive text messages to reduce mood symptoms and problem drinking in patients with primary depression or alcohol use disorder: protocol for an implementation research study.JMIR Res Protoc. 2015 May 15;4(2):e55. doi: 10.2196/resprot.4371. JMIR Res Protoc. 2015. PMID: 25979786 Free PMC article.
-
Use of general practitioners versus mental health professionals in six European countries: the decisive role of the organization of mental health-care systems.Soc Psychiatry Psychiatr Epidemiol. 2013 Jan;48(1):137-49. doi: 10.1007/s00127-012-0522-9. Epub 2012 May 31. Soc Psychiatry Psychiatr Epidemiol. 2013. PMID: 22644000
References
-
- Fernandez A, Haro JM, Martinez-Alonso M, Demyttenaere K, Brugha TS, Autonell J, et al. Treatment adequacy for anxiety and depressive disorders in six European countries. British Journal of Psychiatry. 2007 Feb;190:172–3. - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV. Washington DC: American Psychiatric Association; 1994.
-
- Regier DA, Narrow WE, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Archives of General Psychiatry. 1993 Feb;50(2):85–94. - PubMed
-
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Archives of General Psychiatry. 1994 Jan;51(1):8–19. - PubMed
-
- Offord DR, Boyle MH, Campbell D, Goering P, Lin E, Wong M, et al. One-year prevalence of psychiatric disorder in Ontarians 15 to 64 years of age. Canadian Journal of Psychiatry. 1996 Nov;41(9):559–63. - PubMed
LinkOut - more resources
Full Text Sources
