

Impact of prior HAART use on clinical outcomes in a large Kenyan HIV treatment program
- PMID: 19601781
- PMCID: PMC2735680
- DOI: 10.2174/157016209788680552
Impact of prior HAART use on clinical outcomes in a large Kenyan HIV treatment program
Abstract
Background: HIV treatment programs in Africa typically approach all enrolling patients uniformly. Growing numbers of patients are antiretroviral experienced. Defining patients on the basis of antiretroviral experience may inform enrollment practices, particularly if medical outcomes differ.
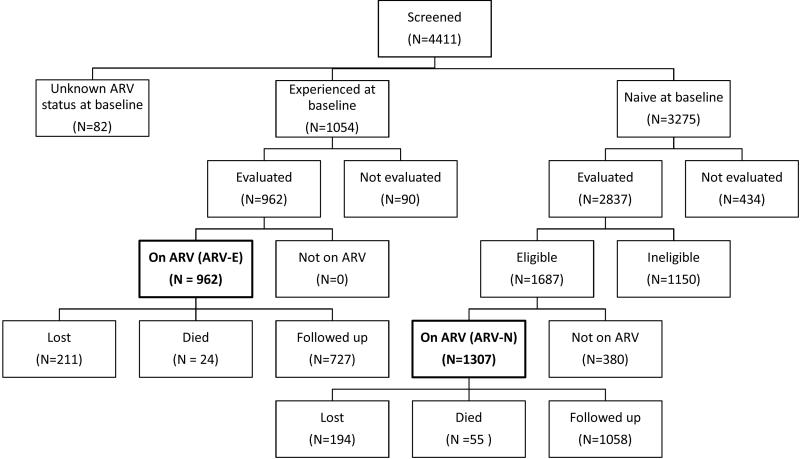
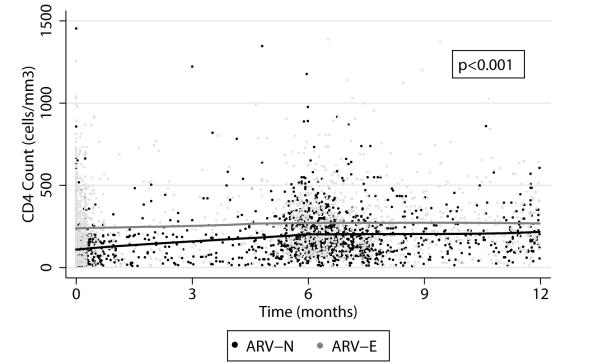
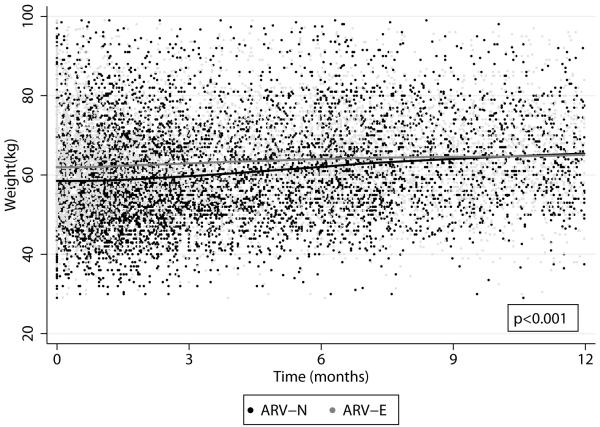
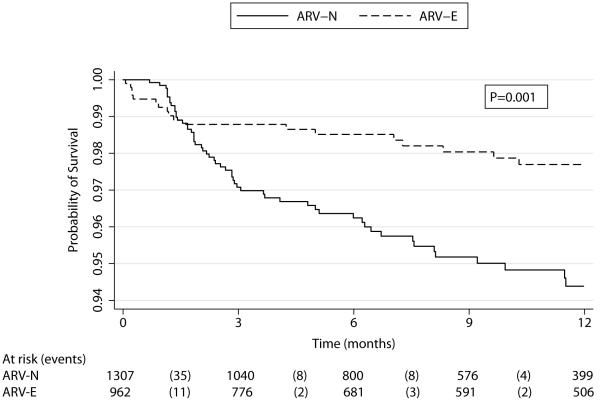
Methods: Baseline and follow-up measures (CD4, weight change, and survival) were compared in a retrospective analysis between antiretroviral-naïve (ARV-N) and antiretroviral experience (ARV-E) patients enrolled at the Coptic Hope Center for Infectious Diseases in Nairobi, Kenya and followed between January 2004 and August 2006.
Results: 1,307 ARV-N and 962 ARV-E patients receiving highly active antiretroviral therapy (HAART) were followed for median of 9 months (interquartile range: 4-16 months). Compared to ARV-N, ARV-E had substantially higher CD4 count (median cells/mm(3), 193 versus 95, P < 0.001) and weight (median kg, 62 versus 57, P < 0.001) at baseline, and lower rates of change in CD4 (-9.2 cells/mm(3)/month; 95% CI, -11.4 -7.0) and weight (-0.24 kg/month; 95% CI, -0.35 - -0.14) over 12 months. Mortality was significantly higher in ARV-N than ARV-E (P = 0.001).
Conclusions: ARV-E patients form a growing group that differs significantly from ARV-N patients and requires a distinct approach from ARV-N clients. Systematic approaches to streamline care of ARV-E patients may allow focused attention on early ARV-N clients whose mortality risks are substantially higher.
Figures
Similar articles
-
Time to viral load suppression in antiretroviral-naive and -experienced HIV-infected pregnant women on highly active antiretroviral therapy: implications for pregnant women presenting late in gestation.BJOG. 2013 Nov;120(12):1534-47. doi: 10.1111/1471-0528.12226. Epub 2013 Aug 7. BJOG. 2013. PMID: 23924192
-
Predictors of mortality in HIV-1 infected children on antiretroviral therapy in Kenya: a prospective cohort.BMC Pediatr. 2010 May 18;10:33. doi: 10.1186/1471-2431-10-33. BMC Pediatr. 2010. PMID: 20482796 Free PMC article.
-
Efficacy and tolerability of nevirapine- versus efavirenz-containing regimens in HIV-infected Thai children.Int J Infect Dis. 2008 Nov;12(6):e33-8. doi: 10.1016/j.ijid.2007.10.008. Epub 2008 Jun 24. Int J Infect Dis. 2008. PMID: 18573672 Clinical Trial.
-
HIV update: emerging clinical evidence and a review of recommendations for the use of highly active antiretroviral therapy.Am J Health Syst Pharm. 2004 Oct 1;61 Suppl 3:S3-14; quiz S15-6. doi: 10.1093/ajhp/61.suppl_3.S3. Am J Health Syst Pharm. 2004. PMID: 15503932 Review.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
Cited by
-
Risk Factors for Hypoxia and Tachypnea Among Adolescents With Vertically-acquired HIV in Nairobi.Pediatr Infect Dis J. 2017 Apr;36(4):e93-e97. doi: 10.1097/INF.0000000000001453. Pediatr Infect Dis J. 2017. PMID: 27977561 Free PMC article.
-
Oligonucleotide ligation assay detects HIV drug resistance associated with virologic failure among antiretroviral-naive adults in Kenya.J Acquir Immune Defic Syndr. 2014 Nov 1;67(3):246-53. doi: 10.1097/QAI.0000000000000312. J Acquir Immune Defic Syndr. 2014. PMID: 25140907 Free PMC article.
-
Cost-effectiveness of cervical cancer screening and preventative cryotherapy at an HIV treatment clinic in Kenya.Cost Eff Resour Alloc. 2017 Jul 14;15:13. doi: 10.1186/s12962-017-0075-6. eCollection 2017. Cost Eff Resour Alloc. 2017. PMID: 28725164 Free PMC article.
-
The consequences of post-election violence on antiretroviral HIV therapy in Kenya.AIDS Care. 2011 May;23(5):562-8. doi: 10.1080/09540121.2010.525615. AIDS Care. 2011. PMID: 21293984 Free PMC article.
-
Increasing HIV-1 pretreatment drug resistance among antiretroviral-naïve adults initiating treatment between 2006 and 2014 in Nairobi, Kenya.AIDS. 2016 Jun 19;30(10):1680-2. doi: 10.1097/QAD.0000000000001110. AIDS. 2016. PMID: 27058353 Free PMC article.
References
-
- Katabira ET, Oelrichs RB. Scaling up antiretroviral treatment in resource-limited settings: successes and challenges. AIDS. 2007;21(Suppl 4):S5–10. - PubMed
-
- Fairall LR, Bachmann MO, Louwagie GM, et al. Effectiveness of antiretroviral treatment in a South African program: a cohort study. Arch Intern Med. 2008;168:86–93. - PubMed
-
- Severe P, Leger P, Charles M, et al. Antiretroviral therapy in a thousand patients with AIDS in Haiti. N Engl J Med. 2005;353:2325–34. - PubMed
-
- Stringer JS, Zulu I, Levy J, et al. Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. JAMA. 2006;296:782–93. - PubMed
-
- Wools-Kaloustian K, Kimaiyo S, Diero L, et al. Viability and effectiveness of large-scale HIV treatment initiatives in sub-Saharan Africa: experience from western Kenya. AIDS. 2006;20:41–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
