

Role of EG-VEGF in human placentation: Physiological and pathological implications
- PMID: 19602057
- PMCID: PMC6512391
- DOI: 10.1111/j.1582-4934.2008.00554.x
Role of EG-VEGF in human placentation: Physiological and pathological implications
Abstract
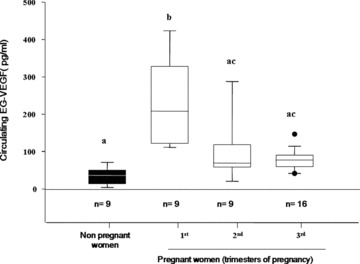
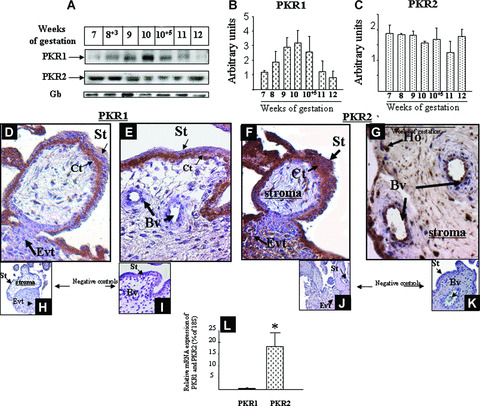
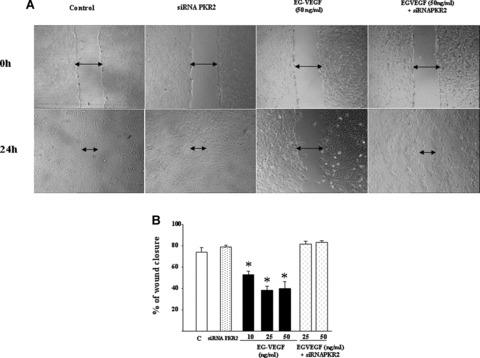
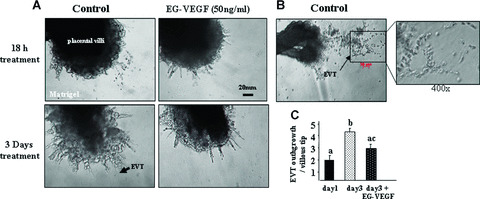
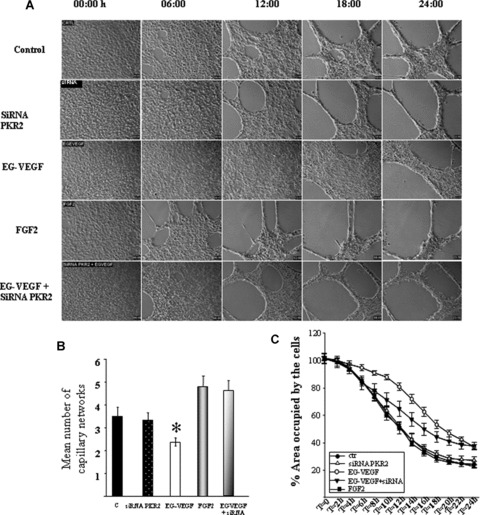
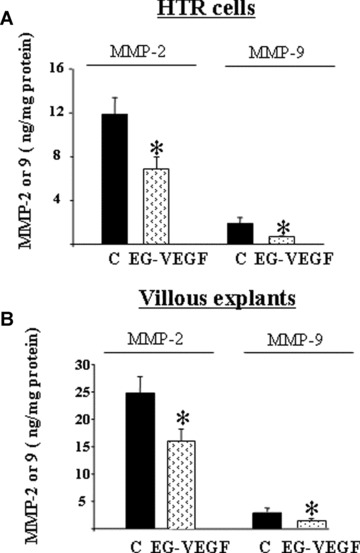
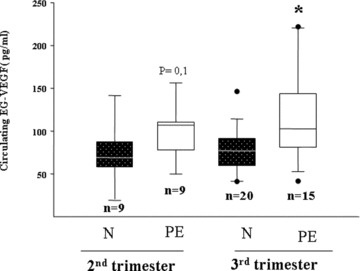
Pre-eclampsia (PE), the major cause of maternal morbidity and mortality, is thought to be caused by shallow invasion of the maternal decidua by extravillous trophoblasts (EVT). Data suggest that a fine balance between the expressions of pro- and anti-invasive factors might regulate EVT invasiveness. Recently, we showed that the expression of the new growth factor endocrine gland-derived vascular endothelial growth factor (EG-VEGF) is high in early pregnancy but falls after 11 weeks, suggesting an essential role for this factor in early pregnancy. Using human villous explants and HTR-8/SVneo, a first trimester extravillous trophoblast cell line, we showed differential expression of EG-VEGF receptors, PKR1 and PKR2, in the placenta and demonstrated that EG-VEGF inhibits EVT migration, invasion and tube-like organisation. EG-VEGF inhibitory effect on invasion was supported by a decrease in matrix metalloproteinase (MMP)-2 and MMP-9 production. Interference with PKR2 expression, using specific siRNAs, reversed the EG-VEGF-induced inhibitory effects. Furthermore, we determined EG-VEGF circulating levels in normal and PE patients. Our results showed that EG-VEGF levels were highest during the first trimester of pregnancy and decreased thereafter to non-pregnant levels. More important, EG-VEGF levels were significantly elevated in PE patients compared with age-matched controls. These findings identify EG-VEGF as a novel paracrine regulator of trophoblast invasion. We speculate that a failure to correctly down-regulate placental expression of EG-VEGF at the end of the first trimester of pregnancy might lead to PE.
Figures
References
-
- Cross JC, Werb Z, Fisher SJ. Implantation and the placenta: key pieces of the development puzzle. Science . 1994; 266: 1508–18. - PubMed
-
- Strickland S, Richards WG. Invasion of the trophoblasts. Cell . 1992; 71: 355–7. - PubMed
-
- Aplin JD. Implantation, trophoblast differentiation and haemochorial placentation: mechanistic evidence in vivo and in vitro. J Cell Sci . 1991; 99: 681–92. - PubMed
-
- Sibai B, Dekker G, Kupferminc M. Pre‐eclampsia. Lancet . 2005; 365: 785–99. - PubMed
-
- Wells M. The pathology of gestational trophoblastic disease: recent advances. Pathology . 2007; 39: 88–96. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
