

Effectiveness of imiquimod limited to dermal melanoma metastases, with simultaneous resistance of subcutaneous metastasis
- PMID: 19602071
- PMCID: PMC2904832
- DOI: 10.1111/j.1600-0560.2009.01290.x
Effectiveness of imiquimod limited to dermal melanoma metastases, with simultaneous resistance of subcutaneous metastasis
Abstract
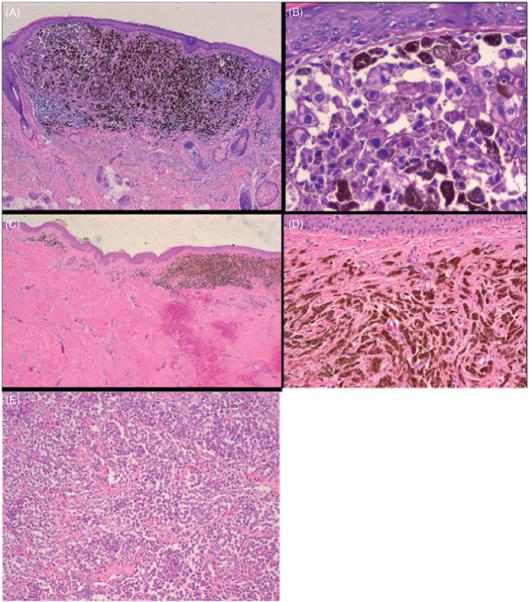
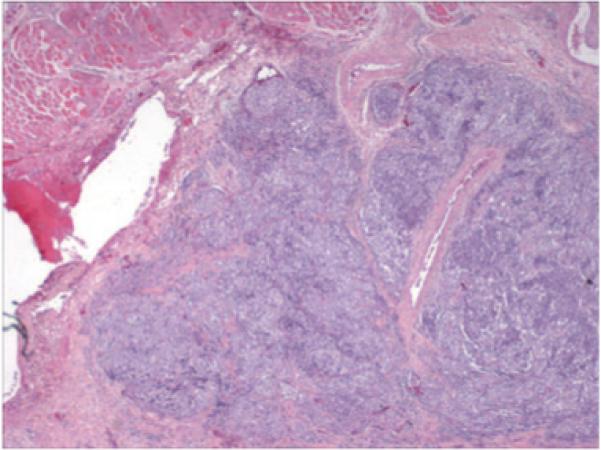
Successful management of epithelial skin cancers with imiquimod 5% cream (Aldara), an immunomodulatory agent, led to speculation that it may promote an immune response against melanoma. Studies, mostly case reports, have assessed the value of imiquimod as a topical treatment for dermal melanoma metastases that prove difficult to manage surgically. The precise value of imiquimod, however, in treatment of dermal and subcutaneous metastases remains unclear. A case at our institution elucidates histopathologically that subcutaneous metastases may progress despite excellent treatment of superficial dermis in the same location. In preparation for a clinical trial using imiquimod to treat patients with dermal melanoma metastases, we have treated several patients off protocol. We present a case report in which the observed changes are documented photographically and histologically. The patient experienced dramatic improvement in the locally treated dermis with concurrent regional treatment failure in the subcutaneous space. Our experience supports growing evidence that imiquimod for some provides an effective option for dermal disease. The unique histological documentation we provide regarding the differential effectiveness of imiquimod in treating various tissue components may help guide future investigations regarding optimal clinical application of imiquimod therapy for melanoma metastases.
Copyright © 2009 John Wiley & Sons A/S.
Figures

References
-
- Woodmansee C, Pillow J, et al. The role of topical immune response modifiers in skin cancer. Drugs. 2006;66:1657. - PubMed
-
- Ugurel S, Wagner A, et al. Topical imiquimod eradicates skin metastases of malignant melanoma but fails to prevent rapid lymphogenous metastatic spread. Br J Dermatol. 2002;147:621. - PubMed
-
- Bong AB, Bonnekoh B, et al. Imiquimod, a topical immune response modifier, in the treatment of cutaneous metastases of malignant melanoma. Dermatology. 2002;205:135. - PubMed
-
- Steinmann A, Funk JO, et al. Topical imiquimod treatment of a cutaneous melanoma metastasis. J Am Acad Dermatol. 2000;43:555. JO. - PubMed
-
- Cotter MA, McKenna JK, et al. Treatment of lentigo maligna with imiquimod before staged excision. Dermatol Surg. 2008;34:147. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
