

Top-down lipidomics reveals ether lipid deficiency in blood plasma of hypertensive patients
- PMID: 19603071
- PMCID: PMC2705678
- DOI: 10.1371/journal.pone.0006261
Top-down lipidomics reveals ether lipid deficiency in blood plasma of hypertensive patients
Abstract
Background: Dyslipoproteinemia, obesity and insulin resistance are integrative constituents of the metabolic syndrome and are major risk factors for hypertension. The objective of this study was to determine whether hypertension specifically affects the plasma lipidome independently and differently from the effects induced by obesity and insulin resistance.
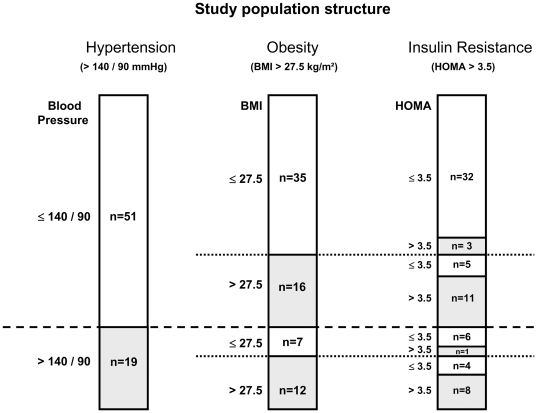
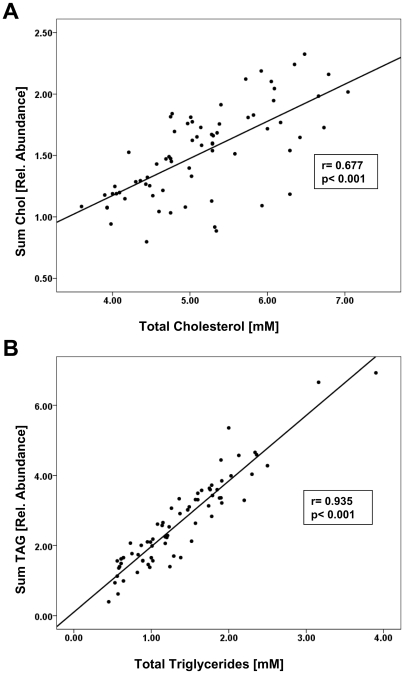
Methodology/principal findings: We screened the plasma lipidome of 19 men with hypertension and 51 normotensive male controls by top-down shotgun profiling on a LTQ Orbitrap hybrid mass spectrometer. The analysis encompassed 95 lipid species of 10 major lipid classes. Obesity resulted in generally higher lipid load in blood plasma, while the content of tri- and diacylglycerols increased dramatically. Insulin resistance, defined by HOMA-IR >3.5 and controlled for BMI, had little effect on the plasma lipidome. Importantly, we observed that in blood plasma of hypertensive individuals the overall content of ether lipids decreased. Ether phosphatidylcholines and ether phosphatidylethanolamines, that comprise arachidonic (20:4) and docosapentaenoic (22:5) fatty acid moieties, were specifically diminished. The content of free cholesterol also decreased, although conventional clinical lipid homeostasis indices remained unaffected.
Conclusions/significance: Top-down shotgun lipidomics demonstrated that hypertension is accompanied by specific reduction of the content of ether lipids and free cholesterol that occurred independently of lipidomic alterations induced by obesity and insulin resistance. These results may form the basis for novel preventive and dietary strategies alleviating the severity of hypertension.
Conflict of interest statement
Figures





References
-
- Castelli WP, Anderson K. A population at risk. Prevalence of high cholesterol levels in hypertensive patients in the Framingham Study. Am J Med. 1986;80:23–32. - PubMed
-
- Neutel JM, Smith DH. Hypertension: where have we gone wrong and how can we fix it? Am J Hypertens. 1998;11:150S–157S. - PubMed
-
- Reaven GM. Relationship between insulin resistance and hypertension. Diabetes Care. 1991;14(Suppl 4):33–38. - PubMed
-
- Bo S, Gambino R, Gentile L, Pagano G, Rosato R, et al. High-normal blood pressure is associated with a cluster of cardiovascular and metabolic risk factors: a population-based study. J Hypertens. 2009;27:102–108. - PubMed
-
- Nguyen NT, Magno CP, Lane KT, Hinojosa MW, Lane JS. Association of hypertension, diabetes, dyslipidemia, and metabolic syndrome with obesity: findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J Am Coll Surg. 2008;207:928–934. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
