

The hepatic response to thermal injury: is the liver important for postburn outcomes?
- PMID: 19603107
- PMCID: PMC2710295
- DOI: 10.2119/molmed.2009.00005
The hepatic response to thermal injury: is the liver important for postburn outcomes?
Abstract
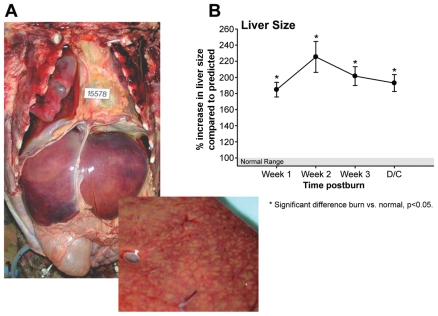
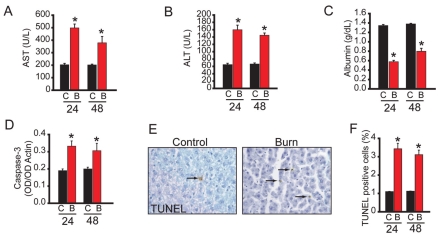
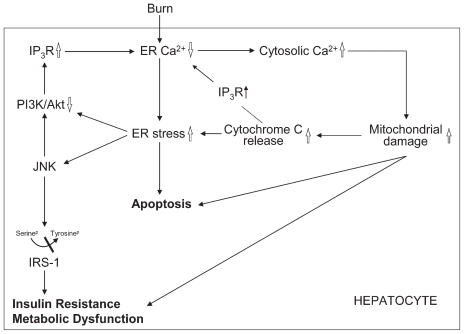
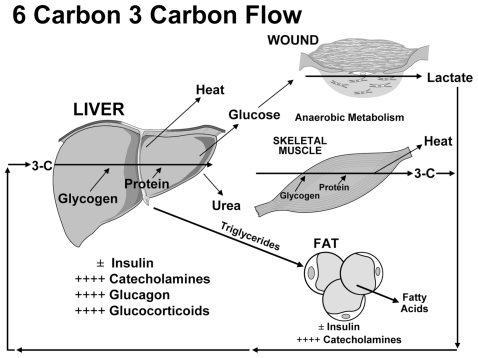
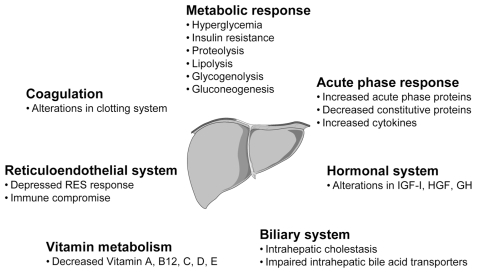
Thermal injury produces a profound hypermetabolic and hypercatabolic stress response characterized by increased endogenous glucose production via gluconeogenesis and glycogenolysis, lipolysis, and proteolysis. The liver is the central body organ involved in these metabolic responses. It is suggested that the liver, with its metabolic, inflammatory, immune, and acute phase functions, plays a pivotal role in patient survival and recovery by modulating multiple pathways following thermal injury. Studies have evaluated the role and function of the liver during the postburn response and showed that liver integrity and function are essential for survival, and that hepatic acute phase proteins are strong predictors for postburn survival. This review discusses these studies and delineates the pivotal role of the liver in patients following severe thermal injury.
Figures
References
-
- Bringham PA, McLoughlin E. Burn incidence and medical care use in the United States: estimates, trends and data sources. J Burn Care Rehabil. 1996;17:95–107. - PubMed
-
- World Health Organization. Facts about injuries: Burns. Geneva: WHO, Injuries & Violence Prevention, Non-Communicable Diseases and Mental Health; [place unknown]: International Society for Burn Injuries; (WHO), Injuries & Violence Prevention, Non-Communicable Diseases and Mental Health; p. 5. No date. Listed as a 2004 fact sheet at: http://www.who.int/violence_injury_prevention/publications/other_injury/....
-
- Palmieri TL, Greenhalgh DG. Topical treatment of pediatric patients with burns: a practical guide. Am J Clin Dermatol. 2002;3:529–34. - PubMed
-
- Nelson KJ, Beierle EA. Exhaust system burn injuries in children. J Pediatr Surg. 2005;40:E43–6. - PubMed
-
- Foglia RP, Moushey R, Meadows L, Seigel J, Smith M. Evolving treatment in a decade of pediatric burn care. J Pediatr Surg. 2004;39:957–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
