

Levels of C-reactive protein associated with high and very high cardiovascular risk are prevalent in patients with rheumatoid arthritis
- PMID: 19606218
- PMCID: PMC2707000
- DOI: 10.1371/journal.pone.0006242
Levels of C-reactive protein associated with high and very high cardiovascular risk are prevalent in patients with rheumatoid arthritis
Abstract
Objective: C-reactive protein (CRP) levels>3 mg/L and>10 mg/L are associated with high and very high cardiovascular risk, respectively, in the general population. Because rheumatoid arthritis (RA) confers excess cardiovascular mortality, we determined the prevalence of these CRP levels among RA patients stratified on the basis of their RA disease activity.
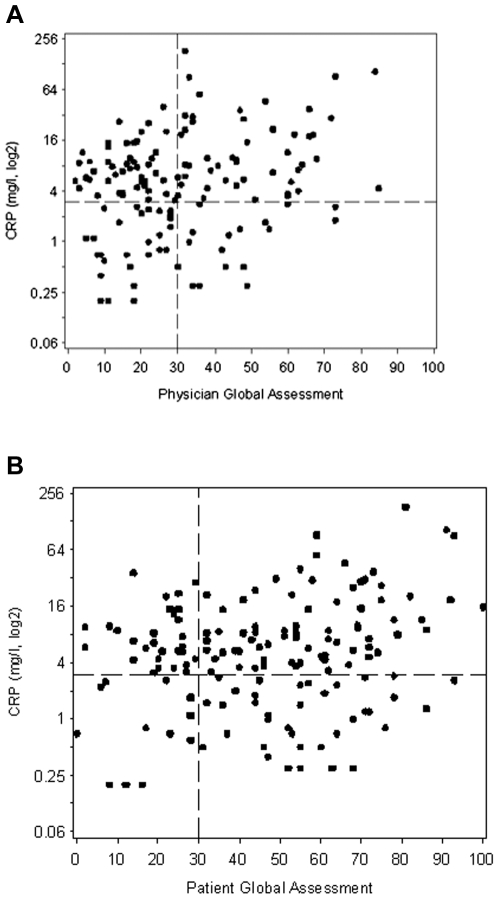
Methods: We evaluated physician and patient global assessments of disease activity, tender and swollen 28 joint counts, erythrocyte sedimentation rate (ESR), and CRP measured in a single clinic visit for 151 RA patients. Disease activity was calculated using the Clinical Disease Activity Index (CDAI) and the Disease Activity Score 28 Joints (DAS28-ESR and DAS28-CRP).
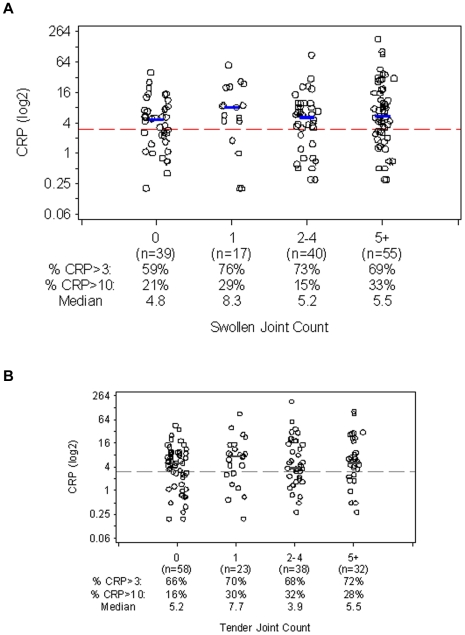
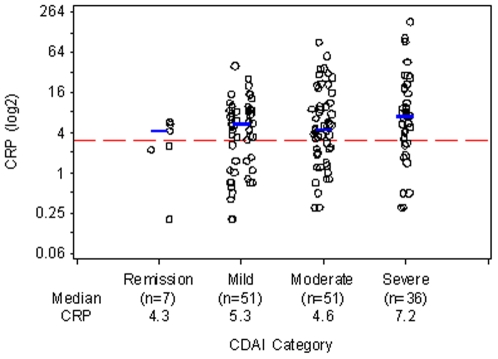
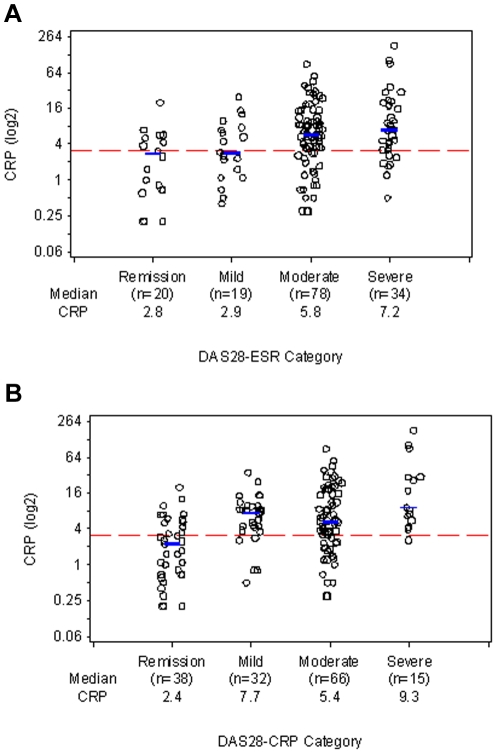
Results: Median CRP level was 5.3 mg/L. 68% of patients had CRP>3 mg/L, and 25% had CRP>10 mg/L. Of those with 0-1 swollen joints (n = 56), or 0-1 tender joints (n = 81), 64% and 67%, respectively, had CRP>3 mg/L, and 23% and 20%, respectively, had CRP>10 mg/L. Of those with remission or mildly active disease by CDAI (n = 58), DAS28-ESR (n = 39), or DAS28-CRP (n = 70), 49-66% had CRP>3 mg/L, and 10-14% had CRP>10 mg/L. Of patients with moderate disease activity by CDAI (n = 51), DAS28-ESR (n = 78), or DAS28-CRP (n = 66), 67-73% had CRP>3 mg/L, and 25-33% had CRP>10 mg/L.
Conclusion: Even among RA patients whose disease is judged to be controlled by joint counts or standardized disease scores, a substantial proportion have CRP levels that are associated high or very high risk for future cardiovascular events in the general population.
Conflict of interest statement
Figures
References
-
- Maradit-Kremers H, Crowson CS, Nicola PJ, Ballman KV, Roger VL, et al. Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: a population-based cohort study. Arthritis Rheum. 2005;52:402–11. - PubMed
-
- Book C, Saxne T, Jacobsson LT. Prediction of mortality in rheumatoid arthritis based on disease activity markers. J Rheumatol. 2005;32:430–4. - PubMed
-
- Young A, Koduri G, Batley M, Kulinskaya E, Gough A, et al. Mortality in rheumatoid arthritis. Increased in the early course of disease, in ischaemic heart disease and in pulmonary fibrosis. Rheumatology. 2007;46:350–7. - PubMed
-
- Solomon DH, Karlson EW, Rimm EB, Cannuscio CC, Mandl LA, et al. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis. Circulation. 2003;107:1303–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
