

Varicella zoster virus vasculopathies: diverse clinical manifestations, laboratory features, pathogenesis, and treatment
- PMID: 19608099
- PMCID: PMC2814602
- DOI: 10.1016/S1474-4422(09)70134-6
Varicella zoster virus vasculopathies: diverse clinical manifestations, laboratory features, pathogenesis, and treatment
Abstract
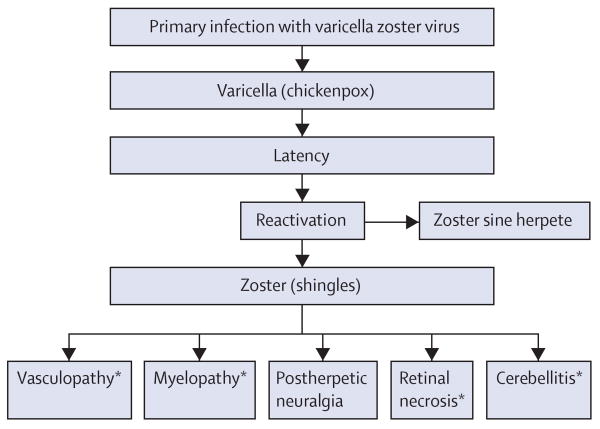
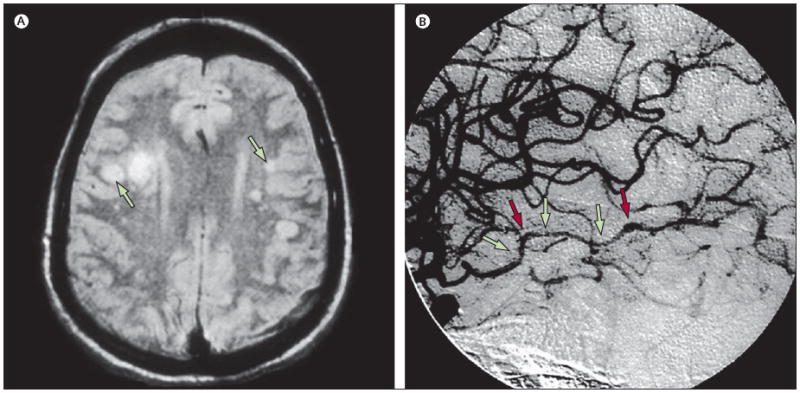
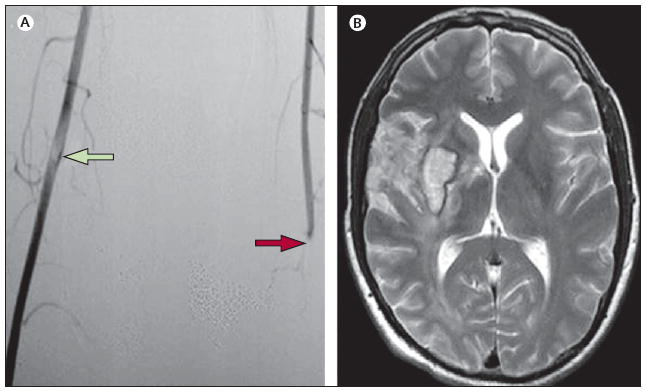
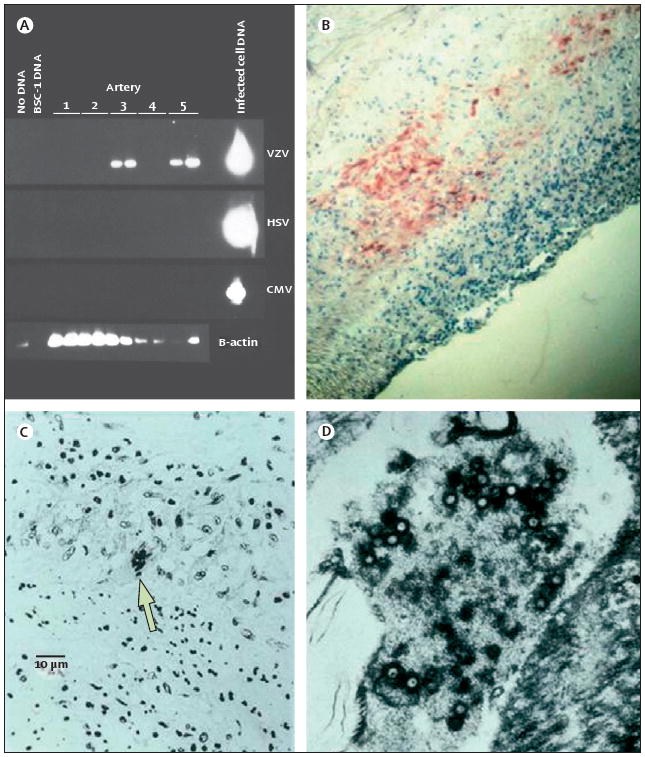
Vasculopathies caused by varicella zoster virus (VZV) are indicative of a productive virus infection in cerebral arteries after either reactivation of VZV (shingles) or primary infection (chickenpox). VZV vasculopathy can cause ischaemic infarction of the brain and spinal cord, as well as aneurysm, subarachnoid and cerebral haemorrhage, carotid dissection, and, rarely, peripheral arterial disease. VZV vasculopathy in immunocompetent or immunocompromised individuals can be unifocal or multifocal with deep-seated and superficial infarctions. Lesions at the grey-white matter junction on brain imaging are a clue to diagnosis. Involvement of both large and small arteries is more common than that of either alone. Most patients have a mononuclear cerebrospinal fluid pleocytosis, often with red blood cells. Cerebrospinal fluid pleocytosis and rash are absent in about a third of cases. Anti-VZV IgG antibody in the cerebrospinal fluid is found more frequently than VZV DNA. In recent years, the number of recognised VZV vasculopathies has grown, and accurate diagnosis is important for the effective treatment of these disorders.
Conflict of interest statement
Figures

References
-
- Askalan R, Laughlin S, Mayank S, et al. Chicken pox and stroke in childhood. A study of frequency and causation. Stroke. 2001;32:1257–62. - PubMed
-
- Cravioto H, Feigin I. Noninfectious granulomatous angiitis with a predilection for the nervous system. Neurology. 1959;9:599–608. - PubMed
-
- Rosenblum WI, Hadfield MG. Granulomatous angiitis of the nervous system in cases of herpes zoster and lymphosarcoma. Neurology. 1972;22:348–54. - PubMed
-
- Gilbert GJ. Herpes zoster ophthalmicus and delayed contralateral hemiparesis. Relationships of the syndrome in central nervous system granulomatous angiitis. JAMA. 1974;229:302–04. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
